Here, four surgeons review the latest thinking on how best to use today’s cutting-edge technology to achieve the outstanding results your patients are expecting.
Measuring Axial Length
Certainly the most significant change in the measurement of axial length has been the shift from ultrasound to laser interferometry, or optical biometry. “Today, more than 80 percent of the surgeons I talk to are using optical biometry to measure axial length for lens power calculation,” says Jack T. Holladay, MD, MSEE, FACS, clinical professor of ophthalmology at Baylor College in Houston. “That means they’re using either the Lenstar or the IOLMaster, the latter being the original optical biometer on the market. About 90 percent of eyes can be measured using optical biometry; only a dense, central cataract will force the surgeon to rely on ultrasound to make the measurement.”
“Biometry is not just about measuring from the tear film to the back of the eye any more,” notes Michael E. Snyder, MD, who practices at the Cincinnati Eye Institute and is a volunteer assistant professor at the University of Cincinnati School of Medicine. “It’s measuring all of the different interfaces that we encounter between the tear film and the back of the eye. For example, the Lenstar uses laser interferometry to measure corneal thickness, anterior chamber depth (defined as the distance from the front of the cornea to the front of the lens), aqueous depth (the distance from the back of the cornea to the front of the lens) and lens thickness.
|
Dr. Snyder notes that these measurements have become increasingly useful. “Latest-generation IOL power formulas such as Olsen’s formula now incorporate lens thickness and anterior chamber depth, increasing their accuracy,” he says. “Also, having measurements such as corneal pachymetry can be clinically useful. Sometimes a patient who’s in the clinic for a cataract consult has a high pressure reading. If the laser biometry measurements have already been obtained, I can review the pachymetry; if the cornea is thicker than average, I know the measurements made by applanation tonometry are going to be higher than the actual pressure.”
Dr. Holladay notes that optical biometry has two advantages over ultrasound. “The first is that it measures to the fovea because the patient is fixating on a target when you take the measurement,” he says. “Ultrasound measures to the posterior pole, which is the longest part of the eye, a little more nasal. In long eyes, that’s clearly not the right measurement, because the foveal measurement would be much shorter. It makes far more sense to measure the optical axial length than the anatomic axial length.
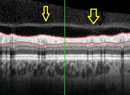
“The other big advantage of optical biometry is that it takes retinal thickness into account,” he continues. “Ultrasound only measures to the internal limiting membrane, which is the anterior part of the retina. The photoreceptors are deep in the retina, so you have to add about 200 µm to an ultrasound measurement in order to account for retinal thickness—and retinal thickness can vary from 160 to 400 µm, so 200 µm is just a guesstimate. With optical biometry, you’re measuring the actual thickness of the retina to the point you want. These two factors have led to a significant improvement in our axial length measurement when using optical biometry.”
Refining Axial Measurement
Dr. Holladay notes that the precise measurement of axial length is not a simple feat, and it continues to be refined. “About two years ago, Doug Koch and Li Wang wrote an article showing that optical biometry has one of the same problems we encounter using ultrasound for this measurement,” he says. “Historically, the ultrasound measurement has assumed an average velocity for the sound as it travels through the different media—cornea, aqueous, vitreous and lens—usually 1,555 meters per second. In reality, the velocity of sound through each of those media is different.
“Using an average velocity to calculate the distance traveled may provide an accurate result in an average eye, but it can confound the measurement in a very long or short eye,” he continues. “The same thing is true of the index of refraction when measuring with optical biometry; the index of refraction is different for the cornea, the aqueous, the vitreous and the lens. Just as ultrasound used an average sound velocity, the IOLMaster and Lenstar use an average index of refraction. However, in long eyes the light spends a much smaller percentage of the time traveling through the lens than in an average eye, and the result is an overestimation of the axial length in long eyes.
“What Drs. Koch and Wang’s article showed,” he says, “was that the average being used produces an accurate measurement in an average eye with a 4.7-mm thick lens and an axial length of about 23.5. However, the measurement in a long eye might say the axial length is 33 mm when it’s really only 32. That incorrect measurement will cause you to underpower the IOL and get a significant hyperopic surprise.”
Dr. Holladay explains that to compensate for this, Drs. Wang and Koch developed a conversion adjustment for the axial length in eyes over 25 mm that can be plugged into the Holladay I or II, SRK/T or Hoffer Q formulas to correct for the error. “It’s called the Wang-Koch axial length adjustment over 25 mm,” he says. “It tells you what axial length to put into the formula to come up with the target refraction you’re aiming for. Currently, none of the instruments are making this correction for you, so using the Wang-Koch conversion formula is the best way to avoid hyperopic errors today. We’ve incorporated it into our Holladay IOL Consultant program [at hicsoap.com] as well, to help ensure that surgeons using the IOL Consultant get the right lens power for extremely long eyes.”
Dr. Holladay adds that ultrasound still has a place in the measurement of axial length. “Ten percent of patients cannot have accurate optical biometry measurements,” he points out. “You have to be able to see the macula to get a good measurement. If you can’t see it, neither can the instrument. You can’t even get a good optical biometry measurement in a patient who has a 3- to 4-mm, dense posterior subcapsular cataract, because it blocks the center pathway. The light then takes an oblique path around the cataract and ends up giving you a longer-than-actual length. Basically, if you find you’re getting a low signal-to-noise ratio, you should be suspicious of your measurement and switch to ultrasound.”
Keratometry Considerations
“We used to think of keratometry as strictly guiding us in the selection of the implant lens power,” says Dr. Snyder. “Today, keratometry also helps us determine what kind of astigmatism we’re dealing with and whether we want to adjust for it. We have to make sure our measurements account for astigmatism, because patients now expect both power and astigmatic accuracy. They certainly need to be offered the option of having their astigmatism corrected.
|

One issue when measuring with keratometry is that each instrument measures the cornea somewhat differently, altering the result. “Manual keratometry still measures a 3.2-mm ring; the IOLMaster measures a 2.5-mm ring; the Lenstar averages a 2.35-mm and 1.65-mm ring measurement together,” says Dr. Holladay. “They all give a different measurement of the same cornea, although in a normal person, the differences would be insignificant—less than a quarter-diopter. That’s not the case, however, if the cornea has undergone surgery such as LASIK. LASIK treatments are not constant across the treated zone; the postop cornea will be a little flatter in the center than at the periphery. So the smaller-diameter instrument will measure a flatter K; the bigger-diameter instrument will measure a steeper K.
“However, no one of those measurement diameters is necessarily any better for measuring the power on a specific patient than another,” he continues. “That’s why you have to personalize things. If you put your postop refractions in after surgery and personalize your lens constant for the instrument you’re using, over time your constant will adjust for the bias of your particular instrument.”
These differences can also affect the astigmatic axis reading. “From a purist perspective, the closer you measure to the center, the more accurate you ought to be,” says Dr. Snyder. “After all, when we use our eyes we’re looking through the center of the cornea. The problem is that none of the current devices is very good at measuring right at the center. They all make assumptions based on the average shape of a cornea. This is especially problematic in terms of determining the astigmatic axis.
“For example, manual keratometry is basically measuring two single points on the cornea at the 3-mm optical zone that are 90 degrees apart,” he continues. “So if you have a tiny variation or some mild irregular astigmatism where one of those two points happens to fall, it can induce a very meaningful artifact. For that reason, I’m not a fan of manual keratometry, except as a double-check. I know that some people still consider manual keratometry to be the gold standard, but I personally do not.
“The IOLMaster measures six points and uses those six points to mathematically compute a best-fit oval,” he says. “The longest axis of that oval is presumed to be the correct axis. But those six points are 60 degrees apart, and this is supposed to determine the axis down to a single degree. The Lenstar has 32 points in two separate concentric circles. This should be more precise, simply because the number of data points is greater. My clinical experience seems to bear this out.
“Some will suggest using corneal topography for this purpose, since it measures hundreds or thousands of data points,” he adds. “As it turns out, that creates a different problem. Astigmatism is very seldom 100 percent regular from the center of the cornea out to the periphery. So the question then becomes, at what distance from the center do you measure the axis? Maybe the axis is at 20 degrees at 2 mm from the center, 18 degrees at 5 or 6 mm out and 12 degrees at 7 mm out. Which axis do you pick? One way to proceed would be to use the points closest to the center, since that’s the part of the cornea our central vision passes through. That’s a good premise, but then you’re basing the axis on a small number of data points again.”
The Cassini Device
Terrence P. O’Brien, MD, professor of ophthalmology and director of the Refractive Surgery Service at Bascom Palmer Eye Institute of the Palm Beaches in Miami, has for several months been using a new device that has recently become available: the Cassini corneal shape analyzer (from i-Optics in Westboro, Mass.). The instrument’s design is reminiscent of a placido topographer, but it uses red, green and yellow LEDs, each one positioned in a unique relationship to four of its neighbors, to project light onto the cornea. Ray-tracing is used to measure the position of each reflected light. According to the company, the multiple colors being used, along with their asymmetric positioning, prevent errors if reflections are smeared or overlapping.
|

“Most ophthalmologists are familiar with placido disc topography, as well as more advanced topographers that use both placido and Scheimpflug technology such as the Galilei system and the Pentacam,” he continues. “Placido-based technology gives us a large number of data points describing the corneal surface, and is typically accurate to within about 0.25 D. However, because placido technology uses concentric rings, it’s easier to measure changes in the radial direction than in any other direction, and source-image mismatches can be a problem.
“This new technology, with its 700 red, yellow and green LED point sources, provides us with more robust imaging,” he says. “The point sources and distinct colors help make sure that there’s no source-image mismatch, and that, combined with its image processing software, makes it especially useful in corneas that are less regular. These are the corneas we most often encounter in eyes that have had prior corneal surgeries, especially LASIK or PRK. The other thing is that the new device has been more repeatable when measuring abnormal eyes. In these eyes, other instruments often yield a range of results when taking multiple measurements.
“We’ve found that for normal eyes, all of these technologies work great,” he adds. “But as the corneal curvature is increased in post-LASIK eyes, the differences among the devices become more apparent, favoring the new device.”
Dr. O’Brien points out a few other advantages of the LED-based instrument. “Cassini’s proprietary image capture and processing are really fast,” he says. “As a result, the image and data are not affected by motion artifacts that can happen if the patient is looking around or has microsaccadic eye movements. We can typically get a good image very rapidly, even in older, less cooperative patients. Also, the 700 points cover a wider swath of the corneal surface than placido. One of the limitations of keratometry is that you’re measuring a small section of the cornea, and with conventional keratometry you’re even missing some of the central cornea. In addition, with some of the placido-based topographers artifacts can occur because of shadows from an eyelash, the nose or even facial features such as high cheekbones. The technology used in the new device is less prone to those kinds of artifacts.”
Dr. O’Brien adds that the Cassini has recently been synchronized with the TrueVision 3-D system. “That’s especially nice to have when implanting a toric IOL,” he notes. “After using the Cassini to measure for a toric IOL, the link allows the TrueVision system to project a virtual image of the astigmatism and where the toric IOL should be aligned onto our surgical view. So instead of using less-than-precise handmade ink marks after measuring with super-expensive, accurate devices, this allows the surgeon to know exactly where to put the toric IOL. I think that’s a big advantage.”
Dr. O’Brien adds that despite the advantages of the LED device, he finds it most useful to combine the information from multiple instruments. “Each technology has advantages in terms of getting the most information about shape and astigmatism and the precise location of astigmatism when screening corneas,” he says. “Each one also has limitations. We’ve found that combining them gives the most information to help with surgical planning, or to help us understand patient dissatisfaction. For example, in post-LASIK or PRK eyes, the Cassini device allows us to measure higher levels of aberration than placido technology, which is helpful in understanding why someone isn’t happy with the quality of his vision. At the same time, adding Scheimpflug to the Cassini gives us more information about the posterior corneal curvature, the anterior chamber depth and so forth.”
Choosing the Right Toricity
|
“For example, suppose you’re dealing with a normal eye that has a 44-D cornea and a 22-D IOL at the normal depth,” he says. “In that situation, you would indeed need a 3-D lens to correct 2 D of corneal astigmatism. But if you have a 34-D IOL, you’ll only need about 2.4 D of correction to offset the 2 D of corneal astigmatism, and if you have a 10-D IOL, you’ll need almost 3.5 D of toric correction in the IOL. And that’s just using the power of the lens as a variable. The IOL will also require more toricity if the cornea is steeper or if the lens is deeper in the eye. All of these variables come into play, so using a single correction factor for every case means you’ll make substantial errors whenever the dimensions of the eye—the K-reading, lens power or IOL distance from the cornea—are not average.”
Dr. Holladay notes that many calculators now take these factors into consideration, including the Holladay IOL Consultant, AMO’s toric calculator and (soon) Alcon’s next generation toric calculator and the Verion System. “However, many other calculators still use a constant,” he says, “so it’s important to be aware that if the eye you’re dealing with is unusual in any way your calculator should take these factors into account. Otherwise, you’re likely to encounter a refractive surprise.
“A second recent refinement in calculating toricity also comes from work done by Drs. Wang and Koch, and it relates to posterior-surface corneal astigmatism,” he says. “When we do keratometry or topography we measure only the front surface of the cornea. Until recently, everyone assumed that if your anterior astigmatism was against-the-rule, any astigmatism on the back of the cornea would also be against-the-rule. In other words, if an eye’s steep meridian was vertical, people expected the steep meridian on the back of the cornea to be vertical as well. It turns out that isn’t true.
“Using Scheimpflug technology, Drs. Wang and Koch have shown that 90 percent of the time, astigmatism on the posterior surface of the cornea is steeper vertically, irrespective of whether the front surface is with-the-rule, against-the-rule or oblique,” he explains. “As a result, it’s the net power of the cornea that matters in our IOL calculations, not the front surface power by itself.
“In practice, this means that if an eye has anterior against-the-rule astigmatism, the vertical posterior cornea is going to exaggerate that, so you should add 0.5 D to your toric IOL correction,” he says. “If the anterior astigmatism is with-the-rule, you should subtract 0.5 D from what you measure with topography or keratometry. If the front surface astigmatism is oblique, say at 45 or 135 degrees, there’s some controversy about what will work best, but most surgeons are basing their calculations on the measured amount, with no adjustment. So far, the data is showing that these corrections are indeed producing better outcomes.”
Dr. Holladay notes that another approach, based on this same insight, is to simply pick the next lower or higher power toricity based on the angle of surface astigmatism. “In other words, if the patient has with with-the-rule astigmatism, go down one toricity power,” he says. “So if you were going to use the T4 lens, you’d go down to the T3. Conversely, and if the eye has against-the-rule astigmatism, you’d move from the T4 up to the T5. This is called the Wang-Koch corneal astigmatism adjustment, and people using this simplified system are also getting improved results.
“It is possible to get an exact measurement so that you don’t have to use a fudge factor, if you have the right technology,” he adds. “We helped develop the Equivalent K-reading that’s available in the Pentacam tomographer, which measures the back surface of the cornea and compensates for it, including any posterior astigmatism. Since the posterior astigmatism is with-the-rule in 90 percent of eyes, 10 percent of eyes will not be served well by the new adjustments [described above]. Using tomography would make sure the net astigmatism was correctly calculated, even in that 10 percent. But you have to have the technology to make that measurement, and even without it your outcomes should be improved in 90 percent of your cases simply by using the Wang-Koch adjustment.”
Dr. Snyder adds a note of caution regarding measuring the posterior surface of the cornea. “The back surface of the cornea is not easily measureable,” he points out. “A few devices in the marketplace do measure the posterior cornea, but whether they’re accurate or not still has to be adequately determined. People consider these measurements the gold standard because they’re all we have at the moment, but I suspect these measurements will get better in the future.”
Intraoperative Aberrometry
Another way to refine cataract outcomes, of course, is to use intraoperative aberrometry to measure the refraction while the patient is aphakic on the operating table (and possibly after the lens has been implanted as well).
“There are two instruments today that provide online, real-time measurement of the refractive error of the eye when the patient is on the operating table: Wavetec’s VerifEye and Clarity Medical Systems’ Holos,” says Dr. Holladay. “This technology allows you to take an aphakic measurement, which Wavetec has shown improves your ability to orient a toric IOL and let’s you refine your spherical power so that more people are within a half diopter of the desired refraction than if you rely solely on preop measurements. This measurement accounts for everything—posterior as-tigmatism, anterior astigmatism, axial length, all of it.”
Despite its advantages, not everyone is sold on this option yet, for a variety of reasons. “Doug Koch has done some fabulous work showing that the posterior surface of the cornea contributes meaningfully to the overall astigmatism of the eye,” says Dr. Snyder. “Given the fact that our measurements of the posterior surface are still unproven in terms of accuracy, intraoperative aberrometry seems like a good way to surmount this concern.
|

“Of course, there is a perfect way to make the measurement,” he notes. “We could get it right every time if we removed the cataract, left the patient aphakic and then brought him back one week later to do the wavefront aberrometry. That’s really the only way to make sure that swelling from hydration doesn’t affect the measurement, but the cost and inconvenience of that would be ridiculous.
“Eventually I believe we’ll all be using this kind of technology, but there’s a lot of refinement that needs to be done,” he concludes. “There are real factors that can alter the measurement that we don’t yet know how to fully compensate for.”
Some surgeons also question whether the extra time and expense required to use this approach is worthwhile, in terms of the number of outcomes that are altered. Dr. O’Brien worked with intraoperative aberrometry for a short time and was not impressed enough to pursue it. “It didn’t seem to make a huge difference,” he says. “On a day with 20 cases, there were only one or two cases where it made a significant difference—but it added a lot of time to each surgery. The OR staff couldn’t understand why we spent 10 minutes on it in every case when it didn’t change the outcome most of the time. And of course, you have to be careful to inflate the anterior chamber to just the right physiologic pressure and shape to ensure an accurate reading.
“Also, do we need this when our measurements on the front end continue to get more robust, more reliable, faster and more reproducible?” he continues. “Plus, intraoperative aberrometry is not reimbursable and the cost is significant. I think the average surgeon is wondering how he can afford a femtosecond laser for cataract surgery, two or three expensive preoperative imaging devices, plus an intraoperative device.”
Dr. Holladay acknowledges that, regardless of its advantages, practical considerations are likely to keep intraoperative aberrometry from replacing the need for preop measurement any time soon. “The preop measurements allow the surgeon to go into surgery with a set of lenses that he’s bracketed to make sure he has what the patient needs,” he points out. “About 60 percent of the time intraoperative aberrometry causes the surgeon to change the choice of lens he was going to use, up or down 0.5 D, so he has to bring six lenses to cover all possible bases. Without a preoperative measurement, he’d have to have access to a complete inventory during surgery, which could be a logistical nightmare.”
|
Optimizing Your Outcomes
These strategies can help you make the most of the current technology:
• Don’t wait any longer to switch to laser biometry. “This technology has been around for many years, and it is superior,” says Dr. Snyder. “Laser interferometry has become the gold standard in axial biometry. It provides the best measurement we can get, while making the fewest possible assumptions. In contrast, ultrasound measurement always depends on whether we’re close enough to the posterior axis, whether there’s a posterior staphaloma or the macula is sloped relative to the instrument. Even the density of the cataract can cause the sound waves to be transmitted differently, leading to an inaccurate calculation of the measurement. Not every eye can be measured with laser biometry, but most can, especially with the newer devices.”
• Use a different personalized A-constant when readings are made by ultrasound vs. laser biometry. “Clinicians sometimes end up looking at records from another practice where the measurements were made using a different technology,” says Dr. Snyder. “Also, some clinicians work in an institution where both ultrasound and laser biometry are in use. In that situation, you need to keep in mind that when using ultrasound, the primary spike gives the measurement to the front surface of the retina, the vitreo-retinal interface. In contrast, laser biometry measures to the retinal pigment epithelium. So, assuming the ultrasound measurement is otherwise perfect, the same measurement made using laser biometry will be longer by the thickness of the retina. Because the average thickness of the macula is only 0.25 mm, you might not think this would make a significant difference, but it can have a meaningful impact. Generally, every millimeter of axial length is equivalent to about 3 D of refractive change. So a quarter of a millimeter error could induce 0.75 D of refractive surprise. To compensate for that you need to have a different personalized A-constant for ultrasound than for laser interferometry.”
• Pay attention to astigmatism. “I believe a discussion of astigmatism correction with every astigmatic patient has now become the standard of care,” says Dr. Snyder. “Skipping this discussion is becoming a challenge for informed consent. I’m not suggesting that every surgeon has to make those corrections; you may feel that your patient population won’t be able to pay for astigmatism correction, so you don’t offer it. If you choose not to correct astigmatism, you can offer to refer to someone else who does. But you need to tell the patient that these technologies exist. Today, excuses won’t cut it with an unhappy patient, and a brief, candid preoperative discussion can save a lot of aggravation.”
• Even if you’re not adjusting for astigmatism, collect the data. “As long as you’re measuring astigmatism preoperatively, you can look at postoperative astigmatic outcomes that correlate with your particular approach so you can best advise your patients on their options and what to expect,” says Dr. Snyder. “That in itself has value.”
• If you can’t acquire laser biometry data in a given eye, use immersion ultrasound, not contact ultrasound. “Immersion ultrasound does not compress the anterior chamber, so the measurements are more accurate and more reproducible than those obtained using contact ultrasound,” says Dr. Snyder. “Of course, immersion may be impossible in some individuals because of orbital anatomy or lack of cooperation. In that case contact A-scan remains the old standby.”
No Perfect Device—Yet
Dr. O’Brien notes that the increasing variety of technologies available to ophthalmologists has become a challenge for many clinicians. “Our group has an advantage, being at a large academic center where we can have several platforms,” he says. “But a person in practice needs to make an informed decision. Everyone has placido technology, but everyone is also aware of its limitations.
“Now clinicians are asking, which of these new instruments should I opt for?” he continues. “Few practices can afford all of them. At the same time, as we move forward with femtosecond laser procedures and toric IOLs—not to mention multifocal toric IOLs—we want the most robust imaging we can get, at the most affordable price. It would be great if one device could do everything and put it all together for us. But anyone waiting to purchase the single perfect instrument will have to wait a little while longer.” REVIEW
Dr. Snyder is a consultant for Haag Streit and Alcon. Dr. O’Brien has no financial interest in i-Optics or the Cassini instrument. Dr. Schallhorn is a consultant for AMO. Dr. Holladay is a consultant for AMO, Alcon, Oculus and Wavetec. He can be reached at docholladay@docholladay.com.