Procedure Volumes
In terms of overall laser vision correction volume, the number of procedures surgeons say they’ve done in the past year has remained constant from last year at 451,000 (339,000 LASIK and 112,000 surface ablation); surface ablation has comprised a quarter of all cases on the survey since 2010. “Even though my practice’s volume has continued to go down, I’m pleased to see that it hasn’t in this cross-section of ISRS members,” avers Mobile, Ala., surgeon Richard Duffey, who administers the survey each year with Palm Springs, Calif., ophthalmologist David Leaming. “I think we’re still suffering a little bit more in terms of the economy in the Southeast, so it continues to go down here while other areas are stabilizing. And, obviously, the volumes of surgeons in some other areas have gone up, on average, along the way.”
Digging into the procedure volumes, in terms of the refractive procedures that surgeons say they perform five or more times per month, toric lenses, presbyopic intraocular lenses and femtosecond cataract lasers (used for refractive purposes) are gaining traction. Half of the surgeons report implanting five or more toric lenses per month; 38 percent say the same for presbyopic IOLs; and 23 percent say they use a femtosecond cataract laser for five or more cases each month. “Those procedures are starting to get some real play in the survey for refractive procedures,” observes Dr. Duffey. “It’ll be interesting to see what happens with those over time. When you get to the question of procedures that are used for 25 or more cases per month, those three categories drop some, with LASIK and surface ablation having the higher percentages. However, 5 percent of the respondents say they do at least 25 refractive cases per month with the femtosecond cataract laser, which is substantial. These are like the early days of laser vision correction, and I think you’ll see great growth in these procedures’ numbers over time.”
A result that Dr. Duffey is particularly impressed by is the proportion of surgeons who either have refractive surgery done either on themselves or their family members. Forty percent of the surgeons on the survey have had it. In terms of surgery for their family members, refractive surgeons report a percentage that’s three times higher than the general population. “If there’s any group that knows the most about it, it’s the refractive surgeons who do it,” says Dr. Duffey.
Treatment Patterns
When it comes to addressing issues such as astigmatism in cataract patients or LASIK flap size, the trend is to try to clean up as much astigmatism as possible and to create thinner LASIK flaps.
|
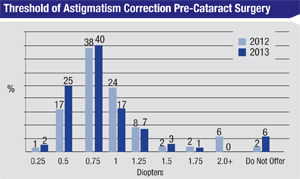
“In terms of the procedures used to correct the astigmatism, on the survey if it’s less than 1 D, 87 percent of the surgeons will do LRIs and AKs,” continues Dr. Duffey. “But, if it’s more than that, 75 percent will use a toric IOL. It will be interesting to see what those numbers do as we get more into femtosecond-assisted cataract surgery. For me, I’ll correct anything under 2 D with the femtosecond laser—because it’s quite effective—before I move onto more expensive toric lens implants. So, it saves the patient some money and I feel I can get close to an equal result.”
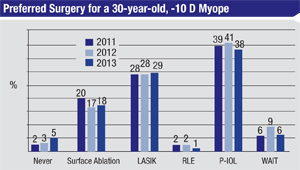
In terms of how surgeons treat high myopia (-10 D or greater), laser vision correction is chosen by 47 percent, versus 38 percent who say they prefer a phakic IOL. “I’m fascinated by the percentage that will do LVC vs. a phakic lens,” says Dr. Duffey. “We all like the idea of staying outside the eye. If I can do it on the surface, I’d much rather do that than place an implant in someone, especially a young patient who’s 30 years old. I’m with the LVC surgeons there.”
 |
One of the possible reasons surgeons are moving toward thinner flaps is to help preserve more corneal strength to ward off ectasia. This fact, as well as the increased use of surface ablation in select patients, may be behind the reason that the survey surgeons aren’t reporting new ectasia cases. Forty-seven percent of surgeons report zero cases of ectasia in their career. “What I’m looking for in ectasia responses on the survey is any real spike that’s consistent over a two- to three-year period and, frankly, I don’t think I’m going to see that,” says Dr. Duffey. “This is because everyone is attuned to ectasia risk now with preop testing, and making thinner flaps to leave more residual bed and/or switching to PRK. Knock on wood, I haven’t seen a case of ectasia since someone I did before 2001 or 2002. I feel confident that we’ve got that problem under control.” REVIEW




