It’s not often that a new excimer laser gets approved for laser vision correction, so when it happens, surgeons take notice. Recently, refractive surgeons were given a new excimer option with the Food and Drug Administration approval of the Alcon/WaveLight EX500 laser, which brings some new features and increased speed to the table. Here’s a look at the new laser and how it might fit into a refractive practice.
Treatment Speed
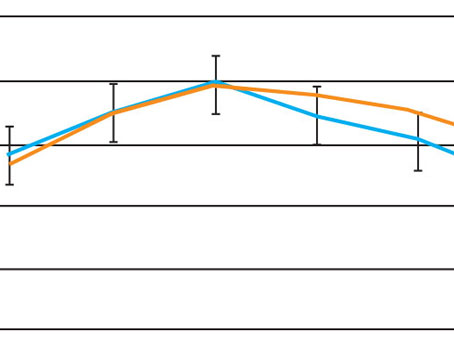
One of the key features of the device is its ablation speed, running at 500 Hz, vs. the speed of the previous model, the Allegretto Wave IQ 400 Hz. “Granted, it’s incrementally faster,” says Greensboro, N.C., surgeon Karl Stonecipher. “However, it matters. With a speed of 400 Hz, the laser ablated at a rate of two seconds per diopter. With 500 Hz, though, it’s speed is 1.4 seconds per diopter.” Dr. Stonecipher says it’s been his experience that up to about -7 D, the outcomes between the 400-Hz and the 500-Hz lasers are somewhat similar. “But when they get out of those treatment ranges into higher ones, as well as with mixed astigmatism and hyperopes, speed becomes a factor, since desiccation becomes important with regard to outcomes.” For comparison, Dr. Stonecipher cites a study that compared the results of the 200-Hz Allegretto Wave to those of the 400-Hz device in 206 eyes of 121 patients with -6 to -12 D of error with up to 3 D of cylinder.1 At the three- and six-month visits in the 200-Hz group, 77 percent (109/141) and 86 percent (121/141) of eyes, respectively, were within ±0.50 D of the intended correction. In the 400-Hz group, 98.5 percent (64/65) and 100 percent (65/65) of eyes were within ±0.50 D of the intended correction at three and six months postoperatively.
In the 200-Hz group, at the three- and six-month follow-up 84 percent (119/141) and 77 percent (109/141) of eyes, respectively, saw 20/20 or better uncorrected. By contrast, in the 400-Hz group 80 percent (52/65) and 92 percent (60/65) of eyes had 20/20 or better uncorrected vision at three and six months, respectively. At the six-month follow-up, Dr. Stonecipher and his colleagues found that refractive predictability and visual acuity were statistically significantly superior in eyes in the 400-Hz group (p<0.01). “We found that the faster 400-Hz results were better, especially with the higher minuses,” says Dr. Stonecipher. “And I think that’s related to speed. This speed also increases your throughput. Some devices run at eight to 10 seconds per diopter, so this can be five times faster.”
Connectivity
The EX500 is also designed in such a way that it fits into a refractive suite of lasers and diagnostic instruments made by Alcon/WaveLight.
“The most interesting thing about the new device, in my opinion, is the connectivity features,” Dr. Stonecipher says.
“You know that the most frustrating thing for us is entering the surgical data. You and your staff have to enter it into the topographer, the tomographer, the computer, the femtosecond laser and the excimer laser. That gets old. Since it takes about one to two minutes per unit, I have to pay someone to sit in front of two computers and put in basic data and information for about half a day on the day before those patients’ surgeries. This new laser has wireless connectivity, so if you use the Alcon topographer, the data you enter into that goes to every other Alcon device in your suite. It’s a huge time saver. Not only does this save time and ensure I’m not losing a staff member for half a day, it also cuts down on data-entry errors.”
|
Accuracy and Safety Measures
It’s common for excimer lasers to allow users to target refractions in increments of 0.25 D. The EX500, however, gives surgeons a little more leeway, allowing them to adjust refractions in 0.01-D increments. It’s possible that such fine adjustments will be able to get patients closer to 20/20 vision.
“Being able to enter refractions in 1/100 of a diopter helps you with the accuracy of your nomogram,” Dr. Stonecipher avers. “In some other systems, if your nomogram called for 2.21 D of correction, you could do a 2-D treatment or a 2.25-D treatment. With this, you can correct the 2.21 D. It will give you that extra edge you might need in order to get closer to the target.”
For surgeons who want to stay on top of even the slightest risk of ectasia, the laser allows them to perform intraoperative, non-contact pachymetry. “It can do the measurements both before the procedure and during it,” says Dr. Stonecipher. “So, for those patients in whom you’re concerned about the depth of the residual stromal bed, you can make intraoperative adjustments. For instance, if you become concerned about the amount of tissue that the laser will have to remove, you can switch from an 8-mm to a 6-mm optical zone.”
The eye tracker runs at 1,050 Hz and has a latency time of 2 milliseconds, tracks pupils from 1.5 to 8 mm and is able to compensate for cyclotorsion.
To be sure to track the eye accurately, the EX500’s tracking system is composed of four lights situated in positions similar to the corners of a rectangle, with a fifth fixation light placed in the middle of the rectangle. The company says that positioning the fixation light within the other lights helps prevent cyclotorsion and gets the eye into the right alignment. The system also allows the surgeon to monitor patient fixation during the treatment, as well.
An Eye Toward the Future
Though they’re not approved in the United States, there are features of the EX500 that are available elsewhere in the world that increase its functionality in various situations.
One of these add-ons is a topography-guided treatment module, which works based on measurements gathered by the WaveLight topographer. The topo-guided treatment is aimed at patients who have asymmetric bow ties, topographic abnormalities, decentrations or need larger treatment zones when there’s a potential for problems with glare and halo. “Outside of the United States, about 85 to 90 percent of cases on the EX500 or Allegretto are performed with a wavefront-optimized treatment,” says Dr. Stonecipher. “Around 10 to 12 percent will be done with the topo-guided treatment. Finally, the use of wavefront-guided is rare with the system, comprising maybe 2 percent of the total.” (For a discussion of topo-guided treatment, see
“Topography-guided Ablation: Pros and Cons,” on p. 20.)
Dr. Stonecipher says WaveLight is looking at ray tracing. “They’re looking at other sources of aberrations and joining them with data points from topography and tomography to try to improve the outcomes of refractive surgery,” he says. “This topo-guided laser platform’s also being used in conjunction with corneal cross-linking to treat keratoconus or laser-induced ectasia, and John Kanellopoulos, MD, has published several papers using the topo-guided laser with his cross-linking treatments. Though our cross-linking studies in the U.S. can only cross-link the patient, in Europe they’re also able to use the laser to correct refractive errors at the same time as the cross-linking.” REVIEW