The Acrysof IQ Vivity (Alcon), Tecnis Eyhance (Johnson & Johnson Vision) and Rayner RayOne (a recent addition that was approved at press time) intraocular lenses were approved by the U.S. Food and Drug Administration this year. The lenses feature technologies not seen in the United States until now: Vivity is the first non-diffractive EDOF lens, and Eyhance and the RayOne are the first approved enhanced monofocals that extend depth of focus. These lenses may broaden the pool of potential candidates seeking greater range of vision, because they’ve each been shown to have low visual side-effect profiles and slightly increased tolerance of mild pathology. In this article, we take a look at the unique designs and features of these lenses.
The Vivity Extended-Vision IOL
Vivity is a novel, non-diffractive extended-depth-of-focus intraocular lens with a 6-mm biconvex, aspheric, wavefront-shaping optic that uses Alcon’s proprietary X-Wave technology. The lens material is a hydrophobic acrylate/methacrylate copolymer with UV and blue light filtration. The lens is available in powers of +15 D to +25 D in 0.5 D increments. It’s also available in a toric version.
Vivity is similar to a monofocal in that it’s non-diffractive and has a comparable visual disturbance profile, but it’s a true extended-depth-of-focus lens with a unique central optic, says Cathleen McCabe, MD, who was part of the FDA clinical trial. Alcon calls this lens a “disruptive” technology, indicated for patients who aren’t suitable for diffractive lenses.1 “We worry about implanting diffractive lenses in patients with pathology, since those lenses split light,” she says. “We don’t have that concern with Vivity.”
Vivity’s Novel Approach
Vivity achieves an extended range of vision by reshaping the wavefront with its central optical element. This element has two features that affect the wavefront differently: elevation and a curvature change. Dr. McCabe explains that the elevation slows down the central wavefront, while peripheral light rays continue to enter the eye and proceed to the retina at the same speed, effectively stretching out the wavefront.
“The peripheral light rays, which focus for distance, reach the retina first, and the folding in of that wavefront, because of the delay in the central portion, extends the focused column of light from distance images outside the 2.2-mm zone all the way to the near-point, somewhere between -1.5 and -2 D,” she says. “That stretched column of precisely focused light allows for a continuous range of vision from distance through intermediate and functional near range.
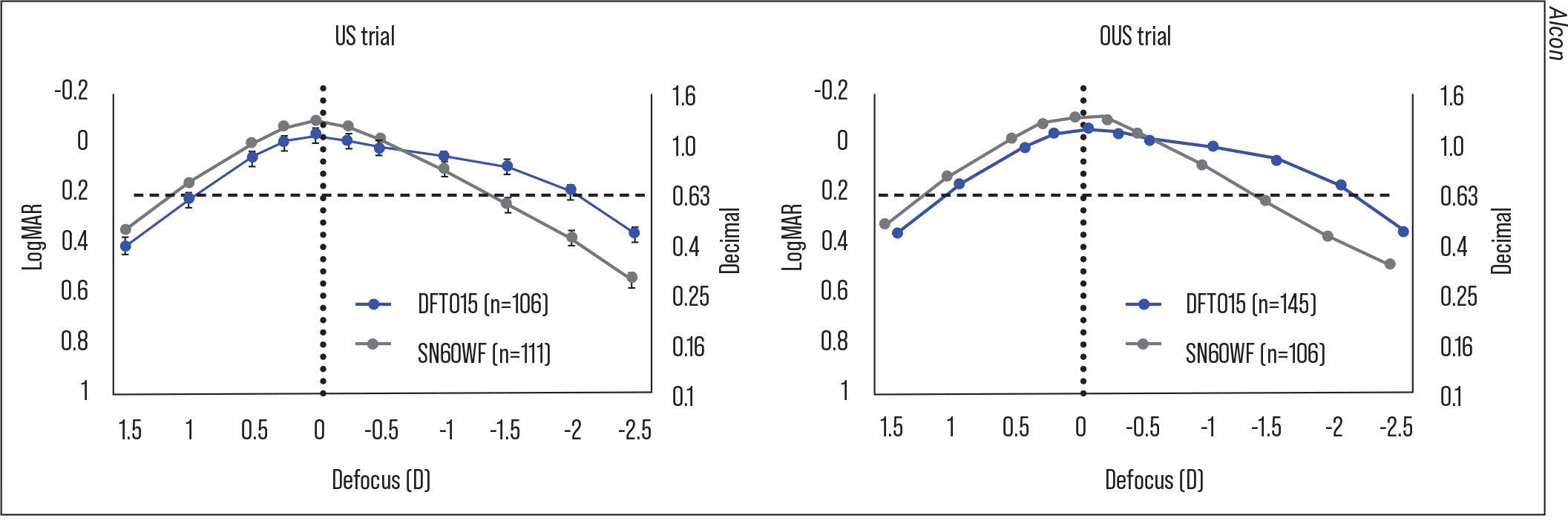 |
| Figure 1. At six months, Vivity provided continuous vision from distance to functional near in both trials. Vivity had a greater negative range of binocular defocus than the monofocal. |
“The light rays in the middle are slowed down, so they come into focus in front of the retina, in the myopic range,” she continues. “If the lens had only this elevation element, it would stretch the wavefront equally in front of and behind the retina. However, all of the light energy focused behind the retina, in the hyperopic range, is unusable. That’s where the second element comes in. The small curvature change in the central 2.2-mm portion of the optic redistributes the light energy that would have ended up behind the retina to the front of the retina. The summation of these two optical elements stretches the wavefront into a longer column of light and shifts the light energy to the functional near focus point instead of behind the retina.”
One of the effects of not splitting light is good image quality. “When light is split, as in a diffractive optic, it’s lost,” Dr. McCabe notes. “For instance, a trifocal lens will use about 50 percent of the light to focus for distance, and 25 percent each for intermediate and near, so if you put a lens like that in a compromised eye, you may not have the image quality that you’d have in a healthy eye.”
The Ideal Vivity Patient
Alcon says that Vivity is suitable for patients with imperfect or healthy eyes who are seeking an extended range of vision. “Vivity performs well in eyes that aren’t pristine; it can provide some near vision, but not spectacle independence,” says John Berdahl, MD, of Vance Thompson Vision in Sioux Falls, South Dakota, who was also involved in the clinical trial. “These lenses are also suitable for patients or surgeons who are intolerant of the potential for dysphotopsias. In my practice, I use Vivity primarily in non-pristine eyes. These are eyes that may have a little irregular astigmatism, some dryness or maybe mild pre-perimetric glaucoma, mild dry AMD or mild epiretinal membrane, but the patients still want some spectacle independence.”
While Dr. Berdahl uses Vivity in less-than-pristine eyes, he says there isn’t currently much data to support this. “You want to be cautious with this lens or any lens in eyes that are diseased,” he says. “Our best data comes from the FDA clinical trial, but our experience so far has been pretty good. I wouldn’t use this lens at first in significantly aberrated eyes or eyes with other significant pathology, however. Get a sense of how the lens performs and then you can consider moving into those more ‘edge’ cases.”
Visual Outcomes with Vivity
Patients implanted with Vivity achieved significantly better intermediate and near vision compared to the SN60WF monofocal in both the US (n=220) and OUS (n=282) trials.
One of the clinical trial findings of particular interest was the amount of good distance vision the lens also provided, says Dr. Berdahl. “Distance vision was as good as the monofocal lens, and that was impressive,” he says.
At six months postop, Vivity provided an improvement of a line or better in binocular distance-corrected, uncorrected intermediate and near vision versus the monofocal. Also at six months, 98 percent, 97 percent and 58 percent of Vivity patients reached 20/32 or better for binocular distance, intermediate and near (near point 40 cm), respectively. Mean MRSE was 0.049 D in the Vivity group (n=107) and 0.081 D in the monofocal group (n=113). Additionally, 91.6 percent of first eyes in the Vivity group were within 0.5 D of target versus 86.5 percent in the monofocal group.2
Overall, patients in the clinical study were satisfied with their quality of vision with Vivity. “The U.S. trial found that 94 percent and 88 percent of patients rated their vision as ‘good/very good’ without spectacles in bright and dim light, respectively, compared to 92 percent and 78 percent, respectively, with the monofocal,” says Dr. McCabe. “I think this line of questioning is a good surrogate for how a lens is actually performing for them at different distances.”
Vivity demonstrated no statistically significant difference from the monofocal in terms of visual disturbances. Two percent and 1 percent of Vivity patients reported that they were bothered “very much” by starbursts and halos, respectively. There were no complaints of glare. Dr. McCabe says complaints were elicited by showing patients pictures of mild, moderate and severe glare, halos and starbursts as reference points. “Because of this questionnaire method, outcomes were reproducible in the OUS and US studies,” she explains. “Numerically, it’s interesting that the starbursts and glare were better in the Vivity than the monofocal lens for both sets of data points, and the halos were slightly more present in the Vivity. But again, none of those were statistically significant differences. Blur, however, was statistically significantly better with the Vivity lens.”
Early Experiences
“One of the interesting things about Vivity is that it has a big plateau of 20/20 or better vision from +0.5 to -0.5 D on the binocular defocus curve,” Dr. McCabe says (Figure 1). “It provides this ‘flexible and forgiving’ plateau of targeting for postoperative refractive error. Because of that forgiveness around plano, Vivity patients had slightly better uncorrected distance visual acuity than the monofocal patients.
“In the US trial we had to choose the target closest to plano, but in the OUS trial they could choose first minus, if they wanted to,” she continues. “With that flexibility in targeting, there were a number of patients who had at least a half diopter of difference between the two eyes, and in that subset of patients they did have an improvement in one line at intermediate and near. Based on that, it seems like mini monovision would be a strategy that would allow for a little enhancement of intermediate and near vision.
“In my practice, I’ve been targeting the dominant eye for plano and the nondominant eye for -0.5 D,” she says. “I’ve had a few patients who ended up slightly more myopic, but I think the sweet spot is around -0.5 D. We’ll have data to back that up when the investigator-initiated trials conclude.”
She adds that because of the plateau around plano, it’s important to push plus in refractions postoperatively. “You can think they’re a little more myopic than they actually are,” she says.
Dr. McCabe points out that Vivity strongly resembles its monofocal cousin, so it’s important to pay attention in the OR, especially when doing high-volume surgery. “It looks like the monofocal in every way until the light reflex from the microscope hits the surface of the lens exactly right—then you can see the central optical element,” she says.
“The bench data for this technology showed that the point-spread function of light distribution is very tolerant of decentration and tilt, but you still want to look for the light reflex so you can center the lens and not mistake it for a monofocal,” she adds. “Postoperatively, it’s kind of the same thing—if the pupil isn’t very dilated and you don’t get the slit lamp exactly at the right angle, it’s hard to see that this lens isn’t just a monofocal. You have to look for that central element.” To view a video of this light reflex, and additional photos, check out the online version of this article at reviewofophthalmology.com.
Eyhance
Eyhance is a one-piece monofocal with a 6-mm biconvex, aspheric anterior surface, made of a UV-blocking hydrophobic acrylic. It features a frosted, continuous 360-degree posterior square edge and C-haptics, offset from the optics. Johnson & Johnson Vision says that this lens provides a 30-percent improvement in contrast in low-light conditions at 5 mm compared to a standard monofocal and has a low dysphotopsia profile, comparable to that of the Tecnis one-piece monofocal. It’s available in powers of +5 D to +34 D in 0.5-diopter increments, and also comes in a toric version.
The lens is one of a new breed of monofocals that offers increased depth of focus compared to standard monofocals. Others include the Xact Mono-EDOF (Santen), which isn’t available in the United States (see sidebar) and RayOne EMV (Rayner), which was approved in late March.
“Eyhance is intended to provide 0.5 D better intermediate vision or 0.5 D better range [than a standard monofocal] at the 20/32 line,” says Daniel Chang, MD, of Empire Eye and Laser in Bakersfield, California. “For reference, the Symfony provides more than 1 D of extended range of vision.”
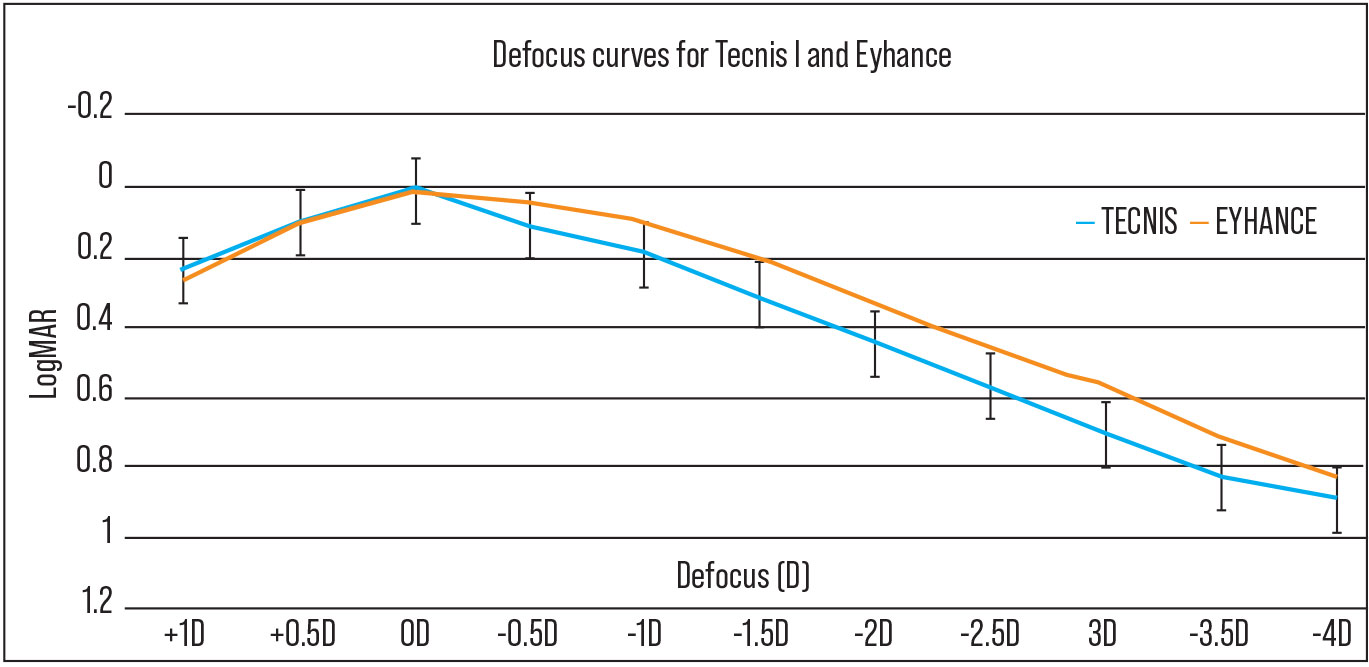 |
| Figure 2. Mean monocular defocus curves for the Tecnis Eyhance (n=71) and Tecnis one-piece monofocal (n=45). Both were similar at 0 D, corresponding to distance (p=0.72). Eyhance had significantly better visual acuity from -0.5 to -4 D and also performed better at intermediate (defocus at -1.5 D) and near (defocus at -2.5 D) distances (p<0.01).7 |
While not an EDOF lens, Johnson & Johnson says Eyhance does deliver true intermediate vision, and that its designation as a monofocal lens will benefit patients looking for more range of vision but who may not be able to afford an EDOF.
Eyhance’s Unique Design
Eyhance’s higher-order aspheric surface produces a change in power without using the diffractive rings commonly seen in many premium IOLs. “Standard aspheric designs predominantly change shape in the peripheral part of the lens, but the higher order asphere in Eyhance is designed to create a smooth and continuous increase in power from the periphery to the center of the lens, as well as continuously change shape in the central part of the lens,” explains Frank Goes Jr., MD, of the Goes Eye Centre in Antwerp, Belgium.
“The higher-order apshere is rotationally symmetric and doesn’t influence asymmetric higher-order aberrations such as coma,” he says. “Eyhance’s periphery is the same as the Tecnis one-piece IOL, and this feature enables both IOLs to reduce spherical aberration to near zero. The two lenses have the same base geometry, and the difference in shape is in the range of microns, which still means a lot for the lens power. Because the power change is continuous, it’s not visible to the naked eye on the lens—i.e., Eyhance doesn’t have any rings or disruptive changes in power. In terms of optical design, both lenses are refractive and reduce spherical aberration to near zero.”
One study analyzing Eyhance’s optical performance reported that the add power in the central 2-mm zone, coupled with the lens’s greater negative spherical aberration values, induced a myopic shift of the maximum optical quality to improve intermediate vision.6 With a 2-mm pupil, the maximum of the through-focus MTFa curve of Eyhance shifted to a myopic defocus of -0.5 D, they reported. For larger pupils of at least 3.5 mm, they found no differences between Eyhance and the ZCB00.6
Eyhance Patient Selection
 |
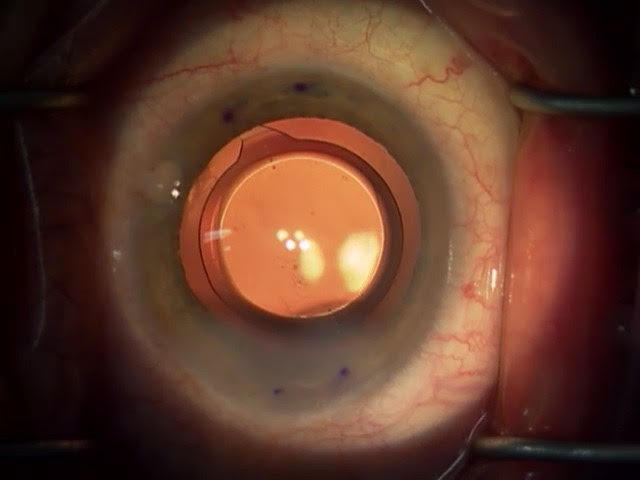 |
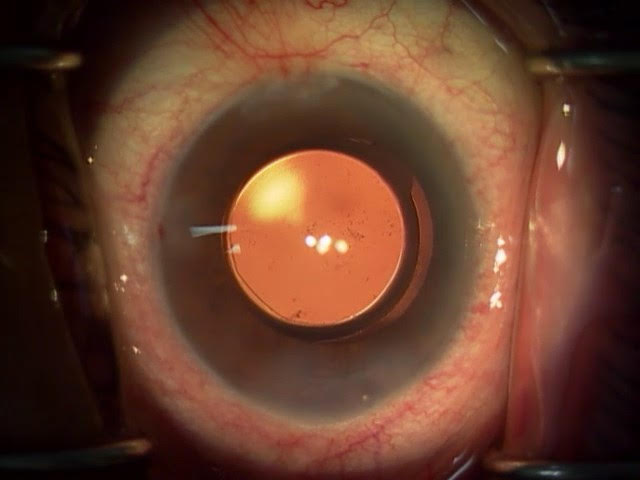
| The DIB00 +17 D (top) and the DIU150 +20 D (bottom). Daniel Chang, MD, says the Eyhance power profile is subtle and cannot be visualized in the surgical microscope. |
Dr. Chang says that Eyhance offers a nice compromise for patients who may not be great candidates for presbyopia-correcting lenses, either because of concurrent pathology or some refractive uncertainty. “It doesn’t compromise image quality, so even patients with some associated pathology will tolerate this lens well,” he says. “I like that I can give them something more than a traditional monofocal or monofocal toric. ”
Oliver Findl, MD, chief of the Institute and chief of the department of ophthalmology at Hanusch Hospital in Vienna, Austria, agrees, noting that his practice has been using Eyhance as its standard monofocal since the spring of 2019. “We’re able to implant this lens in patients with comorbidities such as mild corneal pathology, glaucoma, AMD, DR and DME,” he says. “I wouldn’t expect more visual side effects from this lens, and in the two years I’ve been implanting it, I haven’t encountered those effects.”
Eyhance Studies
Several studies have found that the modified monofocal Eyhance delivers superior intermediate vision compared to standard monofocals.3-5,7,9,11 Three studies found it offered better spectacle independence3-5 and one study found it provided better tolerance of residual refractive error.3
The first study comparing Eyhance (n=80 eyes) to the ZCB00 reported significantly higher uncorrected intermediate visual acuity with Eyhance. Eyhance achieved 0.28 logMAR ±0.11 (Snellen equivalent: 20/38 ±20/25) versus the monofocal’s 0.4 ±0.1 (20/50 ±20/25), p<0.000, for monocular UIVA. For binocular UIVA, Eyhance achieved 0.16 ±0.1 (20/28 ±20/25) versus 0.27 ±0.06 (20/37 ±20/22), p<0.21, with the monofocal.
| OUS Non-multifocal Option for Extending Range of Vision Santen’s Xact Mono-EDOF is a CE-marked monofocal IOL that offers continuous focus from distance to intermediate with a minimal level of glare and halo, according to the company. The 12.5-mm lens is made from the same glistening-free hydrophobic acrylic material as the FDA-approved enVista, but with blue light filtration. It’s available in powers of +10 to +30 D in 0.5-diopter increments. A Phase IV clinical study of 39 eyes of 23 patients reported six-month follow-up data for monocular (n=7) and binocular (n=16) implantation with Xact. Binocular intermediate VA at 50 cm, 60 cm and 70 cm were 20/37, 20/29 and 20/27, respectively. DCIVA and UCIVA values were similar.1
1. New concept monofocal IOL with continuous focus. ESCRS Euro Times Supplement November 2019. Accessed 25 March 2020. https://www.eurotimes.org/wp-content/uploads/2019/11/Santen_Monofocal_Supplement_November2019-Press-Quality.pdf. |
Another independent study found that Eyhance provided better visual acuity than the ZCB00 across a greater range of defocus levels, including near vision.7 Researchers assigned 116 consecutive eyes undergoing phacoemulsification for cataract to either Eyhance (n=71 eyes) or the monofocal (n=45 eyes). The visual acuity target was 0 D, or emmetropia, in both groups. Uncorrected intermediate and near visual acuity were significantly better with Eyhance, with both IOLs demonstrating comparable distance vision results (Figure 2).
A retrospective case-control study published in February comparing Eyhance to the Tecnis PCB00 monofocal found that Eyhance provided a significant improvement in intermediate visual acuity compared to the monofocal without compromising distance vision. The study included 120 eyes of 60 patients (30 in each group) who underwent bilateral cataract surgery. Average binocular UDVA was 20/22 and 20/20 in the Eyhance and PCB00 groups, respectively (p=0.62). Average binocular UIVA was 20/30 in Eyhance and 20/40 in the control (p<0.001). According to the quality-of-life questionnaire administered, Eyhance patients reported less difficulty in performing activities requiring intermediate vision compared to the PCB00.
Eyhance Impressions
“In my experience, patients’ distance visual acuity is similar or identical to that of a classic monofocal lens,” Dr. Findl says. “The need for distance glasses tends to be a little less with Eyhance than with a monofocal lens as well. I believe the reason for this is because Eyhance has a larger landing zone for emmetropia, meaning that if the patient is slightly off-target postop, they’ll still have pretty good unaided vision. This lens seems to have good tolerance to slight deviations in the postop refraction.”
Dr. Goes says that his experience with Eyhance has been similar to the results reported by Professor Gerd Auffarth and his colleagues.8 “I’ve found that Eyhance improves the monocular as well as the binocular DCIVA and UIVA by at least one line on the logMAR scale, while distance vision is comparable to the ZCB00,” he says. “It also has contrast sensitivity comparable to the monofocal and doesn’t have the side effects of multifocal intraocular lenses.”
Eyhance’s similarity to its monofocal cousin makes adapting to this lens easy for surgeons, according to Dr. Findl and Dr. Goes, who note that Eyhance also uses the same IOL constants as the monofocal. “You should treat this lens like a monofocal,” Dr. Goes advises. “It’s very forgiving.” He highly recommends using the max plus technique for refraction.
Because of the forgiving landing zone on the defocus curve, Dr. Chang says you can try two refractive strategies with Eyhance. “This lens has a single wide peak, as opposed to two peaks in its defocus curve, which presupposes some interesting options,” he says. “You could use Eyhance to increase the range of intermediate vision and possibly some near vision, or you could left-shift the defocus curve so you can have some tolerance to refractive error. Eyhance has a smaller peak than the Symfony, so you’d only aim for about +0.25 D hyperopia with this lens. In essence, if you have more variability in the refractive target, you can still maintain good distance vision. The flip side of aiming hyperopic is that you won’t gain intermediate or near vision.”
Breaking News: The RayOne
 |
| The RayONE EMV |
At press time, the RayOne EMV (Rayner Global) received FDA approval from the United States Food and Drug Administration. Rayner says this monofocal offers up to 2.25 D (with 1-D offset) of extended depth of vision. The lens was created for patients desiring spectacle independence who aren’t suitable candidates for diffractive trifocals. Additionally, the company says, “RayOne EMV is a cost-effective solution for patients when diffractive IOLs may be cost prohibitive or if there are concerns about dysphotopsias.”
The 12.5-mm single-piece Rayacryl hydrophilic acrylic lens is available in powers of +10 to +30 D in 0.5-diopter increments in a preloaded intraocular lens injection system.
In a clinical study (n=20), the CE-marked lens demonstrated 20/20 vision in binocular UDVA and dominant eye UDVA, J1/J2 on the Jaeger chart (approximately equivalent to 20/24) for binocular UIVA and 20/32 vision for binocular UNVA.12
These newly approved IOLs are making strides toward what surgeons say is the future standard of IOL technology: lenses with the fewest visual side effects and the greatest range of vision. But as with any refractive procedure, experts say it’s best to under-promise and over-deliver.
“Don’t promise intermediate vision,” says Dr. Goes, referring to the Eyhance, “but do tell the patients that their intermediate vision will be better than it would be with a normal monofocal lens, and that the landing zone of the lens is also
better.”
Dr. McCabe is a consultant for Alcon. Dr. Berdahl is a consultant for Alcon, Johnson & Johnson Vision, Bausch + Lomb and RxSight. Dr. Chang is a consultant for Johnson & Johnson Vision. Dr. Findl is a scientific advisor to Alcon, Carl Zeiss Meditec, Johnson & Johnson Vision, Croma and Merk. Dr. Goes has no relevant financial disclosures.
1. AcrySoft IQ Vivity Extended Vision IOL Product information. FDA.gov. Accessed January 19, 2021. www.accessdata.fda.gov/cdrh_docs/pdf/P930014S126C.pdf.
2. McCabe C. Clinical outcomes of a novel non-diffractive extended vision IOL. International Society of Presbyopia. Presented December 2019. Accessed January 19, 2021.
3. Cinar E, Bolu H, Erbakan G, et al. Vision outcomes with a new monofocal IOL. Int Ophthalmol 2021;41:2:491-8.
4. Unsal U and Sabur H. Comparison of new monofocal innovative and standard monofocal intraocular lens after phacoemulsification. Int Ophthalmol 2021;41:273-82.
5. Mencucci R, Cennamo M, Venturi D, et al. Visual outcome, optical quality, and patient satisfaction with a new monofocal IOL, enhanced for intermediate vision: Preliminary results. J Cataract Refract Surg 2020;46:3:378-387.
6. Vega F, Millán MS, Gil MA, Garzón N. Optical performance of a monofocal intraocular lens designed to extend depth of focus. J Refract Surg 2020;36:9:625-32.
7. Yangzes S, Kamble N, Grewal S, et al. Comparison of an aspheric monofocal intraocular lens with the new generation monofocal lens using defocus curve. Indian J Ophthalmol 2020;68:12:3025-9.
8. Auffarth GU, Geri M, Tsai L, et al. Clinical evaluation of a new monofocal intraocular lens with enhanced intermediate function in cataract patients. J Cataract Refract Surg 2021;47:2:184-91.
9. de Luis Eguileor B, Martínez-Indart L, Martínez Alday N, et al. Differences in intermediate vision: Monofocal intraocular lenses vs. monofocal extended depth of focus intraocular lenses. Arch Soc Esp Oftalmol 2020;95:11:523-7.
10. Petermeier K, Frank C, Gekeler F, et al. Influence of the pupil size on visual quality and spherical aberration after implantation of the Tecnis 1-piece intraocular lens. Br J Ophthalmol 2011;95:1:42-5.
11. Lopes D, Loureiro T, Carreira R, et al. Comparative evaluation of visual outcomes after bilateral implantation of an advanced or conventional monofocal intraocular lens. Eur J Ophthalmol. February 12, 2021. [Epub ahead of print].
12. RayOne EMV: First clinical results. Rayner 2020 Oct.



