The First-Line Agent
Surgeons say that bevacizumab (Avastin, Genentech/Roche), though not officially approved for ocular use, is historically the most-used anti-VEGF agent in the United States. However they add that in some instances they, or their wet AMD patients, feel more comfortable using a Food and Drug Administration-approved agent, either ranibizumab (Lucentis, Genentech/Roche) or aflibercept (Eylea, Regeneron).
“All of us agree that an anti-VEGF agent is the way to go when treating exudative AMD,” says Julia Haller, MD, ophthalmologist-in-chief of the Wills Eye Institute. “So, that’s how we start out. But then the question is: Which agent do you choose? What I’ve found recently, particularly with all the controversy of compounding pharmacies [with bevacizumab] and the like, at least some patients are more interested in going with the FDA-approved drugs, ranibizumab or aflibercept, rather than bevacizumab. It just might be my patient population, but we’re seeing some savvy patients come in and request that they receive a drug that was formulated and packaged specifically for the eye. Now, if there’s a financial issue such as a copay or the like, then, of course there’s no hesitation about using the bevacizumab.”
Philip Rosenfeld, MD, professor of ophthalmology at Bascom Palmer Eye Institute, chooses aflibercept for wet AMD patients that he treats in his hospital-based practice. “When Eylea first came out, I only used it on patients who weren’t responding optimally to Avastin or Lucentis,” Dr. Rosenfeld says. “So my initial experience with it was in that group of patients. But when I saw how well the drug did with them, that’s when I made the decision to use it as initial therapy for my hospital-based patients.”
As to why anti-VEGF agents are the only choice for wet AMD patients, physicians point to high-quality data that has emerged over the past several years on all of the drugs. The National Eye Institute-sponsored Comparison of Age-related macular degeneration Treatments Trials, which were multicenter, prospective, randomized studies, compared ranibizumab to bevacizumab in two different dosing approaches, monthly or p.r.n. The CATT enrolled 1,185 patients.
At two years, the mean increase in letters of visual acuity was 8.8 for monthly ranibizumab, 7.8 for monthly bevacizumab, 6.7 for ranibizumab p.r.n. and five letters for bevacizumab p.r.n. The CATT researchers noted that after adjusting for baseline predictors of visual acuity in a multivariable longitudinal regression model, the estimated change in acuity was 0.7 letters better for ranibizumab in terms of drug (p=0.41) and 1.7 letters better for patients treated monthly in terms of dosage regimen, though the mean visual acuity at two years was similar for all treatment groups at approximately 20/40 (drug p=0.17, dose regimen p=0.41).1
|
In terms of adverse events from the drugs, surgeons say the large-scale studies noted some safety signals, but nothing that would stop anyone from using the agents. In the CATT after two years, the rates of death, heart attack and stroke didn’t differ between bevacizumab and ranibizumab,1 and the VIEW studies didn’t find a difference between aflibercept and ranibizumab in terms of adverse events.2 “People have tried like the dickens to demonstrate an increased risk of heart attack, stroke, thromboembolic phenomena and/or vascular death from Avastin, but they really haven’t found it,” says Dr. Rosenfeld. “I’d argue that if these risks were real, then Eylea, which acts like an antibody and has a much higher affinity for VEGF than Avastin, and which caused adverse events when given systemically in cancer trials, should have demonstrated adverse events when used ocularly—but it hasn’t.”
After reviewing all the data, Wills Eye Institute’s Carl Regillo, MD, doesn’t think there’s an inherent safety issue with the drugs. “I don’t think there’s any difference in safety,” he says. “Unless there’s a compounding pharmacy issue with Avastin, I think all of them are safe, and no real definitive difference between them has come up in clinical studies,” he says. “I think everyone is very comfortable with the safety and efficacy profile of Avastin, and it’s definitely comparable to Lucentis and Eylea. Whether it’s exactly the same, we can’t say for sure. Some may look at the CATT results and say that they see some trends that maybe Lucentis works a little bit better or is a little bit safer, but that’s only a ‘maybe.’ Maybe means that nothing emerged as being statistically significant, though people still like to look at some trends, anyway.”
When considering aflibercept, however, surgeons say the dosing schedule may vary when the drug is used in everyday practice. “Eylea costs slightly less than Lucentis,” says Dr. Regillo, who begins patients on either Eylea or Lucentis as first-line therapy. “Because it costs a little less, if it lasts longer then it would be an even greater value. But whether it lasts longer or not is up in the air. Theoretically, based on some of its chemical properties, it should last longer, but there’s no proof yet that it does, though many believe it might last a little longer than Lucentis. If it does last longer, it’s probably by a little bit, but we just don’t have firm evidence that it lasts significantly longer yet.”
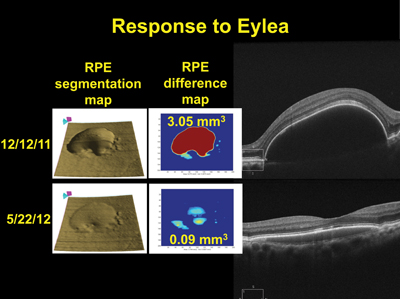
Eylea, by way of relatively small-scale studies, is also gaining a reputation as an effective alternative for patients who don’t respond well to Lucentis or Avastin. In one Phase IV controlled clinical trial, for example, 45 patients with recalcitrant wet AMD despite treatment received the VIEW bi-monthly dosing regimen. In the patients available for six-month visits, the optical coherence tomography improvement from baseline was -33 µm, and they gained an average of 0.8 letters. (Maldonado ME, et al;IOVS 2013;54;ARVO E-abstract 3800)
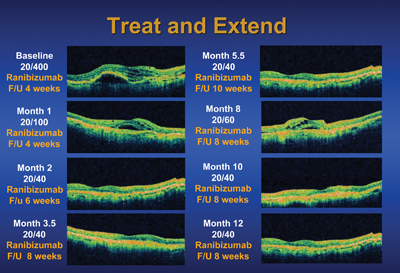
Integral to the efficacy of these drugs, and surgeons’ approach to treating AMD, is the schedule with which they’re injected. Though surgeons may differ on the agent they use first, the one thing most of them agree on, at least according to the 2012 survey of the American Society of Retinal Specialists, is that a treat-and-extend approach is preferable to either monthly dosing or p.r.n. “Last year’s survey shows that only 9 percent of ASRS members use a monthly or bi-monthly approach,” says Dr. Regillo. “Though most of us were using p.r.n. treatment for years, it’s falling out of favor, and only 24 percent use it on the survey. Data such as the two-year results from CATT and IVAN are showing us that, in the long run, p.r.n. doesn’t really stack up well against monthly therapy. It looks good after one year, but after two you can see the results aren’t quite as good. As a result, in comes what most think is the best of both worlds: treat-and-extend, which is used by 67 percent of ASRS members.
“In treat-and-extend, my patients all start the same way: Monthly therapy until the macula is dry,” Dr. Regillo continues. “I treat at the visit at which the macula is finally dry, then extend the patient’s follow-up to six weeks—it’s usually two-week intervals of extension. If he comes back at six weeks and the macula still looks good, I treat and extend him to eight weeks. I keep extending until the disease recurs, at which point I back off on the interval by two weeks and keep him at that resulting interval for a while to minimize recurrences. I might then try to re-extend him later. So, if there’s no activity, you tend to extend. If there is activity, you cut back.”
Avastin: The Low-Cost Leader
Surgeons say financial considerations have always been a fact of practicing medicine, and have become even more significant recently. It’s against this backdrop that Avastin, a dose of which costs about $50 vs. a $2,000 dose of Lucentis—and a fraction of Eylea, which costs slightly less than Lucentis—looms large due to its combination of low cost and good efficacy, despite being unapproved for ocular use.1
“The drug that I use depends on where I am,” says Dr. Rosenfeld. “I have two kinds of practices. One is a hospital-based practice and the other is a provider-based practice. In the hospital-based practice, right now I start with Eylea because, based on analyses we’ve done and papers that have been published, it seems to be a better drug. In my provider-based practice, though, I start them with Avastin. This is because, in a hospital-based practice, Medicare doesn’t reimburse sufficiently for Avastin. This is the result of a ruling back in September of 2009, when Medicare was influenced to stop reimbursement for all Avastin. We were able to get that decision reversed, but only for non-hospital based practices. As a result, CMS only reimburses a hospital-based practice about $7 for the use of Avastin.”
|
Dr. Rosenfeld also makes use of the Chronic Disease Fund, a charity that will provide free drugs to patients who can’t afford them. “In the hospital-based practice, whenever we start using Lucentis or Eylea, we sign patients up with the CDF,” Dr. Rosenfeld explains. “Regeneron and Genentech have an arrangement with the CDF in which the CDF reviews the insurance of the patient, contacts the insurer and determines if the patient qualifies for free drug. I’ll also sign a patient up in the provider-based practice, because if I can’t get him past six weeks without drying the fluid, I’ll try Eylea.”
Though Avastin provides a low-cost option for patients, some physicians are gun-shy of the drug because in order to be used it needs to first be put into single-use syringes by a compounding pharmacy, and this process has resulted in serious infections and vision loss in some patients.3 “The compounding pharmacy issue does factor into Avastin’s safety,” says Dr. Regillo. “You have to realize the product is in someone else’s hands, and there’s the possibility of contamination. So, I use Avastin as second-line.”
Dr. Rosenfeld, though, hasn’t had any problems with Avastin contamination, but says there’s a reason for that. “We’re lucky since we compound our own Avastin, so I haven’t been affected by what’s happened,” he says. “But, if you’re in private practice, you’d better pick a really good compounding pharmacy that you can personally inspect and ensure that it follows Chapter 797 guidelines.” Chapter 797 refers to the chapter on compounding pharmacies in the U.S. Pharmacopeia National Formulary.
Dr. Rosenfeld co-authored a paper on the subject of compounding pharmacies that offered advice on how to choose one:
• Verify the licenses of the pharmacy, the pharmacy manager and its pharmacists via resources on the Web;
• request the last two to three years’ worth of health-department inspections of the facility;
• ensure the preparation area itself is sterile;
• ensure the pharmacists take 10 percent of the batch of drug and incubate it microbiologically, and don’t release the samples for two weeks until they can prove they’re sterile;
• ensure they use a laminar airflow hood in the preparation area; and
• find out if the facility is accredited by the Pharmacy Compounding Accreditation Board, a distinction that shows it’s gone above and beyond the normal certifications.4
“Having a good compounding pharmacy is more expensive,” says Dr. Rosenfeld. “You can’t get a $10 syringe of Avastin; it’s more like $35 if you do it correctly. However, that’s how you have to do it.”
AREDS2 and Good Nutrition
Along with anti-VEGF treatment, physicians say it’s also important to counsel patients with intermediate AMD about the benefits of good nutrition in staving off worse disease.
The latest report from the Age-related Eye Disease Study, AREDS2, was designed to test the effect of the carotenoids lutein + zeaxanthin, the omega-3 fatty acids eicosapentaenoic acid + docosahexaenoic acid or a combination of them on the rate of progression to advanced AMD. They compared the three new formulations to a placebo that consisted of the existing AREDS formula. The study spanned 82 clinics and included 4,203 patients.
The researchers found that when they looked at the entire group and compared approaches that contained lutein + zeaxanthin vs. those without the two carotenoids, there was a 10-percent additional reduction in the risk of progression to advanced disease. This group also had an 11-percent greater reduction in the risk of progression to neovascular AMD in patients who didn’t have choroidal neovascularization at baseline. The researchers didn’t find a beneficial effect with DHA/EPA supplementation. When the investigators looked at the effects of lutein + zeaxanthin vs. beta-carotene supplementation, they found that the former was better, yielding an 18-percent greater reduction in risk of progression to advanced AMD, and a 22-percent greater reduction in the risk of progressing to neovascular disease. In terms of the risk of severe vision loss, the lutein + zeaxanthin formulations produced a 16 percent greater reduction in the risk of losing 30 or more letters, and an 18-percent greater reduction in the risk of becoming legally blind, than the beta-carotene formulation.5
Dr. Haller says AREDS2 has made it easy to discuss nutrition. “I tell my patients that, through AREDS2, we discovered that you can swap out the vitamin A, the beta carotene, which had some risk for cancer in patients who were smokers or previous smokers—and that amounts to a lot of patients,” she says. “We swap in the other carotenoids: lutein and zeaxanthin. I also make sure to note that the omega-3s didn’t show any benefit. I have everyone on the AREDS2 formula, both my wet AMD patients and all my stage-3 dry AMD patients, too.” REVIEW
1. Martin DF, Maguire MG, Fine SL, et al. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: 2-year results: Comparison of age-related macular degeneration treatments trials. Ophthalmology 2012;119:7:1388.
2. Heier JS, Brown DM, Chong V, et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology 2012;119:12:2537-48.
3. Goldberg RA, Flynn HW, Isom RF, et al. An outbreak of streptococcus endophthalmitis after intravitreal injection of bevacizumab. Am J Ophthalmol 2012;153:2:204-208.
4. Gonzalez S, Rosenfeld PJ, Stewart MW, et al. Avastin doesn’t blind people, people blind people. Am J Ophthalmol 2012;153:196-203.
5. Age-Related Eye Disease Study 2 Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: The age-related eye disease study 2 (AREDS2) randomized clinical trial. JAMA 2013;309:19:2005-15.