To say we live in an era of technological change would be an understatement. According to renowned inventor and futurist Ray Kurzweil, personal computers should have computational ability and capacity equal to that of a human being within eight years. (After that ... look out!) We’re not there yet, but every year new technological devices are appearing with greater information capacity, faster computing speeds and ever-expanding capabilities.
One of the most notable developments in recent years has been the advent of handheld computerized devices such as smartphones and electronic tablets. Not surprisingly, ophthalmologists are among those looking for ways to fit these devices into their daily lives—including their practice of medicine.
Mounir Bashour, MD, CM, PhD, FRCSC, FACS, an ophthalmologist and biomedical engineer in Toronto, Ontario, currently medical director at Lasik MD, the largest refractive surgery group in North America, and a long-time early adopter of new technology, notes that the new handheld electronic devices are turning up everywhere. “The hospitals in our area are talking about abandoning their existing pager systems in favor of switching to a smartphone-based system,” he says. “And I recently ate at a restaurant where they hand you an iPad at the table. The iPad shows the menu with pictures of every item. You pick your food and all of a sudden your food materializes. Very cool.” (He adds that the iPads are inside cases that trigger an alarm if you try to take them out of the restaurant.)
Here, a number of practicing ophthalmologists share ways they’ve found to use these devices to make the practice of medicine easier and more effective.
Using the Technology
Doctors are finding a host of ways to use this technology in practice:
• Accessing patient information when away from the office. “I use my iPad for electronic medical records access when I’m offsite at a hospital,” says John S. Jarstad, MD, medical director of Evergreen Eye Centers in Federal Way, Wash., and an adjunct professor at Pacific Northwest University College of Osteopathic Medicine, in Yakima, Wash.
“For example, on a cataract surgery day at the hospital I can review chart notes and preoperative data such as IOLMaster results and astigmatism data. In my own operating room we have a regular desktop computer for accessing patient charts, but in the hospital, I used to have to carry all of the paper charts for the day. And after we switched to electronic medical records, we had to photocopy or print out all of the things we thought we might need during surgery from the patient’s chart—such as the history and physical; the A-scan report; the topography sheets; and the last few eye exams. So the charts got pretty bulky. If you’re carrying 10 or 12 of those to the hospital, you’ve got a pretty heavy briefcase.
|
“Now, I simply access all of the data using my iPad,” he continues. “I just connect with my server at the hospital. There’s an app you can get for about $89—the Pocket Cloud Remote Desktop from Wyse—that lets you connect via the Internet. We haven’t had any security issues so far, and it’s been really reliable. On the downside, there were one or two times I couldn’t get a signal inside the hospital; then I had to call over to the office and have somebody else log in to my account and give me the information I needed. That’s frustrating, but it’s only happened a couple of times.
“Using my iPad for this purpose was a little awkward at first,” he concludes, “but it’s been a really big help.”
• Patient sign-in. Dr. Bashour says that when patients come into the clinic they’re handed an iPad with an online form for them to fill in their information. “The information then goes straight into our patient management system,” he says.
• Smartphone photo documentation. Many surgeons are now using their smartphones to take external photos of patients’ eyes. “I currently take photos with my iPhone and send them to the patient’s EMR for documentation in cases of external disease, tumors and the like,” says Dr. Jarstad. “This is something I hadn’t really thought of until I had to do it one time out of necessity. Someone borrowed the camera we use for taking external photos and took it to one of our satellite offices. So I thought, ‘What can I use to take a photo?’ I realized my iPhone took pretty good pictures, so I used that, and the quality was quite respectable. I’ve been using it ever since.”
|
“I think relying on smartphone photos in some circumstances, such as in the emergency room, is becoming quite common,” says Michael J. Hodkin, MD, an anterior segment and corneal surgeon in Muncie, Ind. “It can be very helpful to have a picture for future reference. If one of my colleagues is going to see the patient in the future, we’ll have a record of what the eye looked like originally. Or it can simply serve to jog my own memory.”
“The quality now is good enough to make it feasible for these applications,” adds Dr. Jarstad. “I could see doing operating room videos with it. That’s probably the next step. You can get upgraded apps for taking higher-definition pictures, and the resolution and definition are probably going to get better and better over time. I’m sure there will soon be all kinds of additional options that we can’t even imagine at the moment.”
• Letting patients send pictures to you. Now that almost everyone seems to have a smartphone with picture-taking capability, some doctors have noted that patients are increasingly using this ability to forward images of their eyes when they have a problem. “Even members of my own family send me pictures of their eye if it’s red or something,” says Dr. Hodkin. “It’s kind of a poor man’s telemedicine. With a smartphone you can take a close-up picture of the eye. It doesn’t always tell the story, but sometimes you’ll get a clue about what’s going on.”
• Accessing textbooks. Dr. Jarstad notes that being able to access textbooks on a smartphone or tablet is very advantageous. “You don’t have to carry around large textbooks, and you can access them from remote locations,” he points out. “That could be especially helpful in the Third World, where physicians and residents may have trouble purchasing expensive textbooks and paying for shipping. Everybody there seems to have an iPhone.”
• Patient education. “We used to have a video player for showing educational videos, but that was a little cumbersome,” says Dr. Hodkin. “A tablet is much easier to manipulate. The patient can watch the video in her lap. It’s also a teaching tool; you can bring up still pictures and explain things. It’s certainly handier than a flip chart.”
“There are times when we use iPads in the exam lane for education,” agrees Dr. Bashour. “You can be interactive when showing patients materials on an iPad. You can use your fingers to expand, move or minify things. It brings you even closer to the patient than doing it on a computer screen.”
• Consent videos. Dr. Hodkin notes that electronic tablets are particularly useful for this purpose. “I’ve made my own consent videos, especially for cataract surgery,” he explains. “Patients watch them either with headphones or without. However, we don’t get their signature electronically. That’s the future, but for now we just have them sign a piece of paper.”
• In lieu of a laptop computer. Dr. Bashour says he almost always uses an iPad now instead of a computer notebook. “The iPad can do 90 percent of what I did on a laptop,” he notes. “For the other 10 percent I use a desktop computer.
“In terms of physical strain, I find these devices less problematic than using a notebook or a desktop,” he adds. “I find the action much more natural. I’ve heard of people having neck pain from looking at devices all the time, but personally I haven’t encountered that.”
• Reading material for the waiting room. Dr. Bashour points out that services are now allowing computer or tablet access to large numbers of popular magazines for a single, inexpensive monthly fee. “I read pretty much all my magazines online,” he says. “People have heard of music services such as Spotify that provide access to everything you could possibly want to listen to for a single monthly fee. There’s now a service doing the same thing for magazines, called Next Issue. For about $10 a month you get access to the current or past issues of about 70 popular magazines. Titles include Car and Driver, Cosmopolitan, Glamour, House Beautiful, Oprah, Popular Mechanics, Vanity Fair, Seventeen, People, Time, Fortune, Better Homes and Gardens, GQ, Esquire, Vogue, Wired and many more. I can just click one and read this month’s issue, or any back issue—and so could patients in your waiting room. I know of doctors who are already doing that, and we’ll most likely try it at some point. With a service like Next Issue, a patient in the waiting room can read whatever he wants.
“Services like this are very democratic, because every time you read something, the appropriate party gets paid,” he continues. “A good article can be read widely without people having to subscribe to a particular magazine. So far, the ophthalmology journals don’t have an equivalent service, but if all the journals related to ophthalmology were available in a single place, all for maybe a few dollars more than a single subscription would cost, it would be extremely convenient for ophthalmologists. It would also be better for the journals, especially the smaller journals, which would be seen by far more doctors. I suspect almost every ophthalmologist would opt for this if it were available. Plus, the journals would know exactly how many eyes are reading every article, which is very valuable information.
“Eventually, I think we’ll see services that, for maybe $200 a month, give you access to everything—all the world’s digital content of every type, all in one place,” he adds. “It’s going to happen sooner or later, and the people who will be most rewarded are those who make it happen sooner.”
Enhancing Your Gadgets
In addition to the possibilities inherent in the devices themselves, special attachments and software can add significant capabilities.
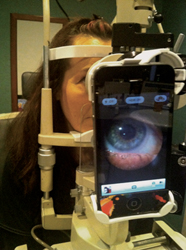
• Smartphone slit-lamp adaptor. One device that Dr. Jarstad has found useful is the Portable Slit Lamp iPhone 4 Imaging Adapter (Keeler Ophthalmic Instruments, $195.00). (See photo, p. 21.)
“This is an attachment for the slit lamp that allows you to use an iPhone to capture slit-lamp photos or videos,” he explains. “I’ve tried it a couple of times, and it works pretty well. Previously, people would try to hold the lens over the ocular in exactly the right position with one hand, then try to focus with the other hand while also keeping the patient’s eye open. Without the device you really need three hands. It’s possible to capture images using your phone without this device, but the attachment makes it much easier to get good, clear photos, in focus. It’s a bit pricey, but it does serve a purpose.”
|

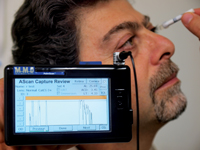
• Pocket A-scan and B-scan devices. Another technology Dr. Jarstad uses when traveling is the PalmScan A2000 A-Scan (from Micro Medical Devices)—a self-contained pocket A-scan on a Palm Pilot platform. (See photo, p. 22.) “It’s like a beefed-up Palm Pilot with an attachment for the A-scan, and it will also do pachymetry,” he notes. “I’ve used that on a couple of mission trips to developing countries including North Korea, Indonesia and the Philippines. It’s nice because it fits in your pocket and doesn’t take up space. It worked superbly and results were very accurate.
“It comes with a little probe that hooks into the top of the device,” he continues. “Then you just take the readings as you would from one of the older A-scans. I think they have an immersion attachment, too. You can run your A-scan calculations and enter your IOL constants and it will give you a printout just as you’d get with a regular A-scan device. It was relatively inexpensive—I think it was a couple thousand dollars. I’m sure something like this will eventually be available for smartphones as well.”
Dr. Jarstad adds that a radiologist he works with has told him about a portable B-scan ultrasound that attaches to the iPhone. “They can use it for obstetrics and other specialties,” he says. “Apparently it works pretty well. It should be a great addition to our medical armamentarium because of its portability.”
• DropBox. Brice R. Nicholson, DO, CDR, MC(FS), USN, a comprehensive ophthalmologist at the Naval Hospital in Bremerton, Wash., says he’s downloaded DropBox software onto all of his computers. “I just started using this recently,” he explains. “It allows me to place documents or photos into a folder, and because it’s cloud-based, I can view and modify the files from any of my other devices. It automatically updates the files on all of the devices as I work on any copy of the file. For example, sometimes I’ll work on a research project at the office, then on my computer at home, then while on vacation or traveling. The DropBox program updates all of the copies at the same time. Furthermore, it saves the old version, so if I realize I deleted something that I need, the earlier version will still be in there. It’s also a great way to share information with others if I wish. It’s very easy to use; it provides 2 GB of space for free; and it works on both PC and Mac computers. I’ve found it to be very helpful.”
Apps, Perhaps?
As everyone knows, part of what makes smart technology so useful is the availability of a seemingly endless supply of applications that allow the technology to perform specific functions. A number of those apps are designed for use by medical professionals. Some favorites include:
• Eye Handbook. Dr. Nicholson finds the Eye Handbook app, developed by ophthalmologists at the University of Missouri Kansas City and Cloud Nine Development, particularly helpful. “It has a wide variety of tools,” he says. “It includes a Snellen-like chart so you can check people’s near visual acuity. It has a pen light if you want to do an exam. It provides information about medications, and you can access the American Academy of Ophthalmology’s Preferred Practice Patterns. It even includes an OKN drum for detecting certain neuro-ophthalmic pathologic conditions. The OKN drum isn’t used as much today as it once was, but it’s one of those tools that every now and then you wish you had.
“I think Eye Handbook is the app I use the most,” he adds. “And they keep improving it with periodic updates.”
• Sight Selector. “The Sight Selector app for the iPad has great pictures and videos you can download onto the iPad for patient education,” says Dr. Nicholson. “It comes with some free basic anatomy photos, but you can purchase specific topics that you might want. My patients like it. I use it on my iPad to show them basic eye information about topics such as astigmatism or the anatomy of the eye. It’s a nice adjunct to the typical globe that we all have in our eye lanes.”
• E-pocrates. “This is a free app for looking up drugs,” explains Dr. Hodkin. “It gives you very complete information on the indications and contraindications, the dosage and the cost, in a very user-friendly format.”
• Podcasts. “Most smartphones have a podcast app,” notes Dr. Nicholson. “You can subscribe to different topics ranging from ophthalmology to non-medical topics. Some of them are peer-reviewed and some have CMEs available. I have Bluetooth in my car, so if I have a 25-minute commute, I’ll listen to podcasts on the way home.”
• Glaucoma 5-Year Risk Estimator. Dr. Nicholson also uses the Glaucoma 5-Year Risk Estimator iPhone app developed with the Washington University School of Medicine in St. Louis. “The ocular hypertension risk calculator is nice for early glaucoma patients with high pressure,” he says. “It lets them know their five-year risk of developing glaucoma.”
• CataractMobile. “A fun no-cost app for Apple and Android tablets is cataractMobile,” says Dr. Nicholson.
“It’s an animated simulator for performing phaco and making capsulorhexis tears. During the making of the ‘rhexis, you put your finger on the touchscreen and it helps you practice your vectors—in other words, where the torque needs to be placed to tear a nice round ’rhexis of a certain size. Obviously there’s no tactile feedback, but it does demonstrate the consequences of grabbing the tissue at different locations and pulling in different directions. It can be a very good adjunct to help beginners get used to those forces—and I think that once you get those forces down, making a great ’rhexis isn’t hard at all.”
• Coding apps. “One type of app I use all the time is for ICD-9 coding,” notes Dr. Hodkin. “It’s basically a database for looking up coding, and there are many apps out there that can help with this. Of course, our techs handle the coding in most situations, but when there’s a question they come to me. These apps help me resolve the tough ones. It’s one of my go-to sources when there’s a coding challenge.”
• The Wills Eye Manual. “It’s the same version as the book, but it’s on the iPhone or iPad,” says Dr. Bashour.
• Lens implant calculators. Dr. Hodkin notes that several of these are available. “An electronic tablet is just as good as a computer for this purpose, but much more portable,” he says. “That makes using it much simpler.”
A Few Suggestions
Surgeons offer some additional strategies for making the most of today’s high-tech handheld technology:
• Use a professional drawing tablet. Smartphones and tablets aren’t the only high-tech devices that can be useful to an ophthalmologist. “My practice is retina-only, so images are a huge part of the practice,” says Steve Charles, MD, FACS, FIC, founder of the Charles Retina Institute in Memphis, Tenn.
“I use a Wacom Cintiq graphics tablet with an LCD display—the one that graphics professionals use. It’s my user interface, my connection to our EMR program.
|

“Some retina specialists make drawings on a piece of paper and then have the drawings scanned in,” he continues. “Or they use programs with small pads and create drawings that don’t really look like the eye. I decided that it made more sense to draw like an artist. This interface can be used two different ways. It has a selection of symbols and colors, so you can use drag-and-drop and create a color-coded drawing that way. Some of my associates do that. I prefer photorealistic drawings, so I use an electronic pen, create the drawings myself, and then do a lot of hand labeling.”
• Have wireless Internet available in your waiting room. “Most of our patients have these devices—even the older folks,” says Dr. Hodkin. “They all sit in the waiting room with readers and so forth. It’s become part of the culture, and everybody’s gotten on the bandwagon. Even our older patients have taken to these devices like ducks to water.
“For that reason, we have wireless Internet in the waiting room, so patients can connect to the Internet with their smartphones or tablets,” he continues. “Having to wait to see the doctor is the most common complaint in most offices. When patients have the opportunity to surf the net on their own device in the waiting room, they have the chance to be productive and/or entertain themselves. They don’t feel like they’re being forced to waste time sitting there, or forced to read our magazines.”
• Consider using an in-office Blackberry-based smartphone system. “We use Outlook and Microsoft Exchange for our in-office communication and e-mail, all connected to an exchange server, making our interoffice e-mail highly secure and HIPAA compliant,” says Dr. Charles. “People seem to be obsessed with iPhones, but Blackberrys do several things better. For example, iPhones don’t talk to the Exchange server as well, and there’s no automatic push of your calendar in an Outlook environment. We have a separate Blackberry Enterprise Server that pushes my calendar and surgery schedule to everyone’s Blackberrys, so all of us see the updated surgery schedule in real-time on our phones. If we need to add a case, everybody can see how full the schedule is.
“I use the same system for my personal calendar, including my travel schedule, but different individuals have different levels of access,” he continues. “Both my assistant and I have read and write access; some others can read my schedule but not alter it. Others, who don’t need to know all of the details of my personal schedule and travel plans, cannot access it. Blackberrys are actually better than iPhones for this.
“Some surgeons say, ‘Oh, I sync our schedules myself,’ but in my office, the second somebody adds something to my calendar, a flight number, an appointment, the time to make a conference call, it’s automatically on my phone and laptop,” he says. “I think that’s far better.”
Concerns and Limitations
Though there’s no end in sight, this technology still raises some concerns, and still has a way to go to fully meet ophthalmologists’ needs. One concern is security—especially important when medical information is involved, and when people are beginning to store information offsite in the cloud.
Dr. Jarstad agrees that this is an issue. “If you store patient information in the cloud, it’s conceivable that someone could hack into the cloud to get digital images of a patient’s eye injury or abuse pictures, something like that,” he says. “But so far the security has been pretty robust. I haven’t seen any issues with that.”
Dr. Charles is skeptical. “Many people seem to be obsessed with the idea of storing information in the cloud,” he notes. “I don’t want to be dependent on communication links and have information stored in far-away places. We don’t use the cloud. We don’t even back up everything at the end of the day. In our office, information is automatically copied onto multiple hard drives in real time.”
Other more basic concerns, such as the possibility of losing a handheld device (or having one stolen) are now being addressed by the devices themselves. “There’s an application from Apple called Find My iPad, or iPhone,” says Dr. Bashour. “I’ve lost my iPhone four or five times, and every time I’ve been able to locate it by logging onto another computer. It tells me where it is. Furthermore, you can send a message that will appear on the screen for whoever finds it; you can lock it down so it can’t be used; and if necessary you can erase everything that’s on it. You can do all of this remotely.”
In terms of limitations, there are a few things the handheld devices don’t seem up to managing, at least so far. For example, some surgeons are now carrying an electronic tablet during exams, but other doctors believe the technology isn’t up to the task. “That’s the last thing in the world I’d want to do,” says Dr. Charles. “In the office I want to have a fixed, great big screen PC that shows every detail of images; one that’s hardwired to the Ethernet, fast as lightning and secure. You don’t have to worry about battery power or carrying it around or people stealing it. I use an iPad for personal tasks outside the office, and it has great features, but I don’t see it as an EMR tool or email
interface. I see it as a specialized tool best used for other purposes.”
Dr. Hodkin agrees that carrying an iPad with you during an exam may be premature. “It doesn’t have enough screen space to do everything we need to do, and the input is more cumbersome because you’re using your fingers instead of a mouse,” he says. “I look at these as niche players for those items that don’t require a lot of input, where portability is the biggest concern. But I think that’s where this is headed.”
The Future of Medicine?
So what does the future hold? “When I first started giving lectures about the wired ophthalmologist back in the 80s, I was considered very far out,” notes Dr. Bashour. “Now, everybody’s connected and using these devices—even ophthalmologists who tend to be late adopters. There’s no question that this kind of technology represents the future of medicine. It’s the future of the world, really.”
Dr. Jarstad does sees cost as a factor in how much this type of technology ends up being adopted. “I think if the manufacturers price things correctly, sales will go through the roof,” he says. “Smartphones are becoming so pervasive in the community that anything that’s really useful will probably be bought by ophthalmologists.
“Truly, a digital revolution is occurring right before our eyes,” he adds. “We’re in a fascinating field, and it’s an exciting time.”
Dr. Bashour agrees. “I love living today,” he says. “It’s pretty amazing.” REVIEW


