For many years, ophthalmologists had few options for treating patients with retinal vein occlusions other than laser and observation. But in recent years, the advent of anti-VEGF drugs and the use of steroids inside the eye have changed that. Currently, anti-VEGF drugs such as ranibizumab and bevacizumab appear to be the most frequently chosen treatment option, but steroids are arguably a good choice in many circumstances. Many surgeons are using them both, either sequentially or simultaneously, and lasers are still part of the equation—sometimes in new ways.
Here, three retina specialists with extensive experience treating central retinal vein occlusion and branch retinal vein occlusion share their thoughts on the pros and cons of steroids, anti-VEGF options and laser, and how they apply these options in the clinic.
The Pharma Approach
David M. Brown, MD, FACS, who practices at Retina Consultants of Houston, helped design most of the major anti-VEGF retinal vein occlusion clinical trials, including BRAVO, CRUISE and COPERNICUS; he was also an investigator in the steroid trials SCORE and GENEVA. “In the past five years we’ve had two big breakthroughs,” he notes. “First, doctors began using steroids in the eye to treat vein occlusion, injecting triamcinolone in the clinic. Then, we began using the anti-VEGF drugs. The latter were initially developed as anti-cancer drugs; then it was discovered that their anti-edema effects in the eye were remarkable. They’re actually much more effective for treating diabetic macular edema, branch retinal vein occlusion and macular degeneration than they are in the cancer realm. Oncologists still use anti-VEGF as an adjuvant, but in our field they caused a revolution.”
| ||||

How the Drugs Work
“Branch retinal vein occlusion and central retinal vein occlusion both cause a breakdown in vascular flow, leading to bleeding and swelling,” explains Dr. Singer. “Because circulation is compromised, this results in ischemia, inflammation and eventually macular edema. Each class of drug attacks one of those problems. The anti-VEGF drugs attack the ischemic component; the steroids attack the inflammatory component. Obviously, there’s a certain amount of crossover, because, for example, VEGF increases the capillary permeability that causes vascular leakage and edema, so decreasing VEGF will lead to some amount of reduction in both edema and inflammation.
“In a vein occlusion, you have a blockage in either the central retinal vein or a branch,” says Dr. Brown. “The eye is a closed-loop vascular system, with arteries that bring in the blood supply and veins that take it back out. Initially we thought that the edema in vein occlusion was at least partly due to increased venous pressure caused by the blockage, but the data from the BRAVO, CRUISE, COPERNICUS and GALILEO trials showed that an anti-VEGF blockade eliminates all the edema within a day or two. That means that venous pressure probably has no role in causing the edema. Instead, blocking venous flow impedes arterial flow, causing ischemia. The ischemic cells then release factors like VEGF and erythropoietin that drive the edematous process.
“Anti-VEGF drugs block that process and make the edema go away,” he continues. “So, if the individual’s poor vision is just due to edema, his vision gets better. In addition, the trial data showed that anti-VEGF treatment also seems to make hemorrhages go away faster. We don’t know whether this happens because the drugs restore the tight junctions of the retinal vessels, or whether macrophages clear the intraretinal hemorrhages faster in a retina that’s thinner and less edematous.
| ||||
“Ultimately, the anti-VEGF drugs work like an antihistamine,” he adds. “If there’s leakage, they stop the leakage. And when they wear off, the leakage starts again."
Dr. Brown explains that the rationale for using steroids to treat vein occlusion is somewhat different. “A steroid also has anti-VEGF effects, although not as strong as the effect of a potent anti-VEGF blocker,” he says. “Perhaps more to the point, steroids help to stabilize retinal vessels’ tight junctions, possibly treating inflammatory activity that happens at the area of the vein occlusion.
“The original histopathological descriptions of vein occlusion done in 1981 by Richard Green, MD, noted that every patient who had a vein occlusion for more than a month had lymphocytic infiltration within the wall of the vein, or into the thrombus,” he adds. “An anti-VEGF drug doesn’t address this. So it may be that a steroid is addressing the root cause of the occlusion in those patients, in addition to its anti-VEGF effects.”
Like many retinal surgeons, Ravi D. Patel, MD, who practices at Retinal Vitreal Consultants in Chicago, says he now relies on the Ozurdex implant when a steroid is called for. “Ozurdex is a bioerodable drug delivery device loaded with dexamethasone,” he explains. “Dexamethasone by itself in the vitreous cavity has a very short life—only four to five hours. But delivered in this polymer implant, the durability is about six months. Data from the GENEVA study [of this implant] showed about a 21-percent gain in three lines in BRVO patients at six months, and about a 17-percent gain in three lines in CRVO patients at six months. Admittedly, if someone just saw those numbers by themselves they wouldn’t be too impressed, but in the past the recommended treatment for CRVO was observation. At least we’re causing improvement.”
“The GENEVA studies show that Ozurdex is a great sustained-delivery platform,” notes Dr. Singer. “The Phase III data shows that at six months vision is still better than with placebo. However, in reality most doctors use Ozurdex as a three or four-month drug. The reason is that the original Ozurdex data didn’t include visits at months four or five, so its performance during that time period was extrapolated.”
Dr. Brown notes another relevant point regarding Ozurdex: The steroid dexamethasone is about five times as potent as triamcinolone, the steroid favored in previous years. “Dexamethasone is 25 times as powerful as cortisone,” he points out. “Triamcinolone is only about five times as powerful. Also, the therapy pulses on and off over time; you get 40 to 45 days of super high-dose steroids and then it pulses off. The evidence suggests that pulse therapy is probably safer for the patient than sustained low-dose steroid. The Alimera implant provided sustained low-dose fluocinolone, rather than pulsed therapy, and it resulted in cataract formation almost 100 percent of the time.”
Anti-VEGF vs. Steroids
With the advent of anti-VEGF options, many retinal specialists have switched from steroids to anti-VEGF.
“Most doctors treating retinal vein occlusion today will initially use anti-VEGF because they get a lot of bang for their buck,” notes Dr. Brown. “You get an eight-letter gain within a week, according to the large clinical trials. If you’re a truck driver and you’re having trouble doing your job, you want that anti-VEGF injection initially. Later, if you’re constantly getting monthly injections, you might be inclined to take a little more risk and go to steroids. Certainly there’s more risk of pressure increase and cataract with use of steroids, although that hasn’t been tested in a standardized fashion.”
“Today, the majority of doctors use anti-VEGF as first-line therapy, primarily because the current studies show anti-VEGF therapy producing superior results compared to Ozurdex,” agrees Dr. Singer. “Some people use Ozurdex as rescue therapy, or when anti-VEGF therapy isn’t producing the desired results. However, Ozurdex does have one significant advantage over anti-VEGF: the convenience factor. You’re not locked into monthly therapy to get those results. In fact, the BRAVO and CRUISE data show that if you only give people three anti-VEGF shots, you lose 20 percent of the improvement you would have seen with all six shots.”
Dr. Brown also notes that the anti-VEGF drugs are an easy sell to most retinal physicians treating retinal vein occlusion. “When you’re a physician, you look at your chances of helping somebody vs. hurting them with a given therapy,” he says. “If you look at the big studies of anti-VEGF therapy, your likelihood of helping somebody is over 99 percent. Your chance of hurting somebody—the risk of endophthalmitis—is about one in 3,000. With steroids, on the other hand, your chance of helping someone may be pretty high—though probably not as high—but your chance of hurting the patient by causing increased IOP or cataract formation is probably one in three. Given that risk-to-benefit ratio, most physicians are going to choose anti-VEGF therapy as first-line therapy. And they’re only going to switch to steroids if they need a lot of anti-VEGF effect to maintain the repression of the edema.
“That being said,” he adds, “in a long-standing vein occlusion, there may be some theoretical benefit to adding a steroid to address the inflammatory component at the actual site of the blockade. In the closed space of the optic nerve head in CRVO and the common adventitial sheath in BRVO, it makes sense that getting rid of the inflammation there might give you a little more flow. It’s worth noting that Richard Green’s histological research found that no one with retinal vein occlusion was totally blocked, so this is a disease of decreased flow, not totally blocked flow. And if there’s inflammation in the wall of the vessel, it’s likely to cause further constriction and impede the flow—at least in theory.
| ||||||||



“The main advantage of a steroid, particularly Ozurdex, is that the anti-VEGFs we have right now are 30- to 60-day drugs, whereas a lot of the steroids give you three or four months’ duration of action,” he continues. “Even though the Ozurdex device probably only gives you high steroid levels for 40 or 45 days, it’s so strong that it calms down the eye and it takes longer for the edema to recur.”
Dr. Brown notes, however, that in his experience Ozurdex doesn’t last six months. “In the Ozurdex trial, most of the patients lost the benefits by six months,” he points out. “So if you compare the Ozurdex results with the BRAVO or CRUISE results, the latter have a 15-letter gain, while the former has lost all of the benefit at six months. Given that, why use Ozurdex? Because when it works—and it often does—you only inject it every three to four months. With anti-VEGF, many patients need a monthly injection.”
Dr. Patel observes that it will be helpful to have direct, head-to-head clinical trial data comparing anti-VEGF treatment to steroids. “They’re now conducting the COMO study in Europe and Israel,” he says. “They’ve enrolled about 400 patients. They’re going to treat with dexamethasone implants at baseline, and again at months five and 10, if needed, vs. monthly ranibizumab injections for six months, followed by as-needed injections through month 12. The primary endpoint will be the mean change in baseline visual acuity at 12 months. I think this study will give us more insight about which drug is superior. Furthermore, sub-analysis may shed light on whether one drug is better than the other for a given population.”
Managing the Steroid Response
One factor that seems to be a primary concern when choosing between anti-VEGF and steroids is the reality that steroids sometimes trigger a belated rise in intraocular pressure, putting some patients in danger of developing glaucoma. ”Nobody wants to talk about it, but it’s clear that the reason most people don’t use steroids is fear of causing glaucoma,” says Dr. Singer. “In that respect, retina specialists aren’t really worried about pressures in the 20s; they’re worried about pressures in the 30s and 40s.”
Dr. Patel notes, however, that in many cases it’s not difficult to know which patients are at risk of a steroid response. “Patients with vein occlusion are often older and have been followed by a comprehensive ophthalmologist for many years,” he points out. “They generally have a good idea of their IOP history. If they’ve had to take steroid drops for a month after cataract surgery, it’s pretty well documented whether or not they are steroid responders. And some patients have a strong family history of glaucoma. In those situations you know that you have to be very careful when using Ozurdex, and I would shy away from it. Ultimately, you have to decide which disease process you primarily want to treat.
“If we decide that Ozurdex is the best treatment option for a patient with a history of glaucoma or known to be a steroid responder, we monitor their IOP very closely,” he says, adding that he relies on his glaucoma-specialist colleagues to help him manage these patients. “Before I start Ozurdex, I send the patient to my colleague for a full glaucoma work-up,” he explains. “I see the patient at six weeks or two months, the period in which the IOP spike typically occurs. To date, when a spike has occurred my glaucoma colleagues have started the patient on an IOP-lowering agent such as Combigan with great success. We’ve never had a case where the IOP was uncontrollable.”
Dr. Singer notes some new developments that may help to lessen doctors’ concerns regarding pressure spikes. “Right now, we’re working on some technology that we presented at the annual meeting of the Association for Research and Vision in Ophthalmology and will be presenting at the meeting of the American Society of Retinal Specialists, showing that we may be able to screen for what I call super-responders—those individuals who will have pressure spikes in response to steroid therapy—using anterior segment optical coherence tomography,” he says. “We may be able to predict who is going to be most vulnerable before any IOP spike occurs. Once you’ve identified them, you can treat proactively with drops or selective laser trabeculoplasty. We’re very excited about this. We hope it will take some of the fear out of using steroids.”
Dr. Singer adds that he chooses SLT to treat steroid super-responders when he encounters them—and has uncovered some new information about how SLT works. “SLT does a great job of preventing steroid-related pressure spikes,” he says. “A study by Ercument Bozkurt, MD, in the American Journal of Ophthalmology in December 2011, showed that by pretreating patients with SLT prior to triamcinolone injection you can prevent an IOP rise.
| ||||||
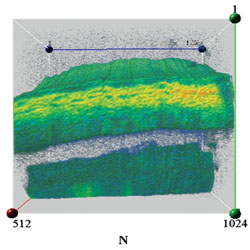
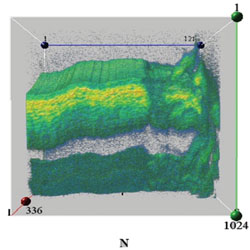
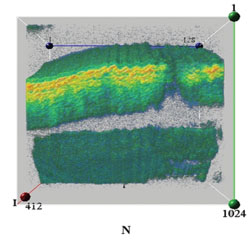
“Meanwhile,” he continues, “our work with in vivo 3-D imaging has revealed some surprising information about what SLT is doing inside the eye. Everyone believes SLT does no damage. In fact, it does cause some mild damage, but the tissue remodels itself within a month. [See images, above.] By the time you look again, you don’t see it. The end result is that performing SLT causes an increase in the angle recess size, lowering the pressure significantly within a week. We’re showing a 3-D movie of this at the major meetings; we were the first people to observe it.
“The bottom line is that if you want to drop the pressure in steroid responders when treating retinal vein occlusion, SLT is the way to go,” he says. “It does it fast and effectively.”
Although fear of triggering a pressure spike is mostly associated with the use of steroids, some recent evidence has indicated that a pressure spike can also happen following anti-VEGF treatment. “A few studies have found that after repeated anti-VEGF injections the trabecular meshwork becomes inflamed on a microscopic level, which prevents the drainage system of the eye from working as effectively as it did before,” says Dr. Patel. “However, only a few small studies have found this; it hasn’t been seen in any large clinical trials. I’ve never had a patient on anti-VEGF drugs whose IOP has become uncontrollable or needed to use topical IOP medications. In fact, I’ve had macular degeneration patients whom I’ve injected with these drugs for the past 30 months who never had an IOP issue.
“Nevertheless, we should be cognizant of that possibility, because it is in the literature,” he says. “However, I’m sure the patients who had those spikes had some predisposing issue or factor or family history that made them more prone to developing the IOP abnormality.”
Perfect Together?
One possibility when considering anti-VEGF and steroid options is to use both. Many surgeons do, combining them in different ways, some sequentially, some simultaneously.
Dr. Patel says he has sometimes combined anti-VEGF and Ozurdex treatments in a single patient. “I do think that’s promising,” he says. “I’ve had a few patients on Ozurdex who seemed to lose their response over time or still had some refractory CME, so I’ve switched them to Lucentis. Over a period of six months I may give them three injections. I’ve also switched to Ozurdex when a patient wasn’t responding as well after six months of Lucentis, or when the patient was tiring of the monthly injections. Either way, making the switch does seem to be effective. There seems to be a symbiotic relationship, where if one drug stops working as effectively as it did initially, the other drug brings back the treatment efficacy.”
“I think a lot of patients would benefit from combination therapy, although very few people do it,” says Dr. Brown. “That’s mainly because the anti-VEGF drugs appear so safe and the patients quickly realize how easy it is to get that 32-ga. injection. In Great Britain where Ozurdex is approved and anti-VEGF is not, there are quite a few doctors using Ozurdex. Next door in Ireland and Scotland, where Lucentis is approved, it’s more like the United States—more people are using anti-VEGF.”
|
“We’ve run a number of clinical trials looking at this type of combination therapy,” he continues. “What’s nice about it, at least in our hands, is that it gives us predictability. When I treat with combination therapy, I can tell you that the macular edema is going to be controlled for about 108 days—three and a half to four months. That’s very consistent from cycle to cycle.
“Basically, I give one shot and two weeks later I give the other shot, for logistical reasons having to do with reimbursement, convenience and so forth,” he explains. “I know with a high degree of certainty that these patients will fall into one of two categories. About 20 percent of them will improve and remain that way for at least six months with just the one treatment. The remainder will get rebound edema three and a half to four months later. What’s remarkable about this is that we can’t make that kind of timing prediction with any other therapy for any other disease. With monotherapy, we can’t be sure how long the improvement will last. But with this combination treatment, we have statistically significant data showing that the timing of rebound edema is predictable.”
Dr. Singer notes that this therapy does require being proactive about a potential steroid response. “In our studies, about 18 to 20 percent of patients have a steroid response to Ozurdex,” he says. “Statistically, it happens between six and 10 weeks, regardless of the magnitude of the pressure spike. So if you want to use combination therapy, you can have the patient seen by a general ophthalmologist or someone in your office to check the pressure at a two-month visit. If the patient happens to be a responder, you can give him a drop and send him on his way. Or, give the patient a drop at the outset and don’t worry about it—although some would consider that overtreating.
“So, if the logistics of monthly injections are too hard for some patients, that’s the conversation I would have with them,” he says. “I explain that they’ll have three sets of combination therapy over the course of a year, and we’ll make sure their pressure is checked at around two months post-injection, just to be safe. Their vision should improve. They may need to use anti-glaucoma drops, but I’ve decreased the number of visits and shots they’ll need.
“Of course, the downside of the combination approach is that patients don’t do quite as well in terms of peak improvement,” he adds. “The GALILEO study showed 17 and 18 letters improvement respectively in central retinal vein occlusion for VEGF-trap at six months. Our data shows somewhere between 13 and 15 letters improvement with combination treatment. So the mean visual acuity gain is slightly less with combination therapy, at least in our hands. However, you do gain convenience. There’s no free lunch—you’re getting one thing in exchange for something else.”
Adding Laser to the Equation
Laser treatment has been used to treat retinal vein occlusion for some time, although without the dramatic results associated with anti-VEGF therapy. Dr. Brown notes that when treating branch retinal vein occlusion, many surgeons add grid laser, particularly in those patients that need continued therapy. “The Branch Vein Occlusion Study data showed pretty convincingly that if you can stop the leakage, using the laser is better than no laser,” he says. “Of course, now that we have anti-VEGF drugs, we protect the fovea by staying outside a 1,500-µm circle. In any case, we haven’t yet seen that tried in combination with anti-VEGF in a clinical trial.”
Today, a number of surgeons are trying a different laser protocol, using it only in the periphery. Early results are promising. “I’ve been giving people anti-VEGF therapy or combination therapy for a number of years now, and the reality is that the majority of people continue to get rebound edema,” says Dr. Singer. “Patients get tired of coming in for shots. The question is, how long will the edema continue to recur in a given patient?
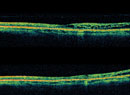
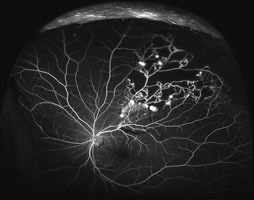
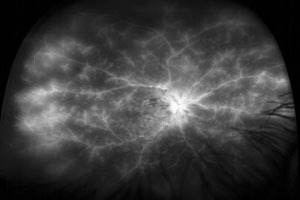
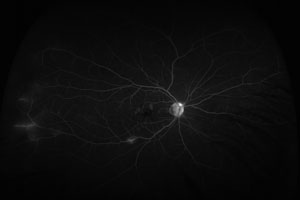
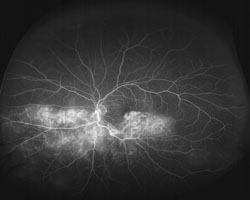
“My experience—and the work of several other researchers—has convinced me that peripheral ischemia is what drives the edema,” he continues. “Our group has recently done some work with widefield angiography using the Optos machine. We’ve been working with the University of California reading center, using very precise algorithms to quantify peripheral ischemia. We found that individuals who have more edema have more peripheral ischemia. And, we’ve found that giving anti-VEGF shots increases circulation, causing a decrease in ischemia that’s accompanied by reduced macular edema.”
Dr. Singer says that, with this finding in mind, they’ve been working to use targeted laser photocoagulation on the peripheral ischemia. “This is not the same as using focal laser to treat the areas of edema,” he points out. “In the Central Vein Occlusion Study, lasering the macula was not significantly better than observation.”
| ||||||
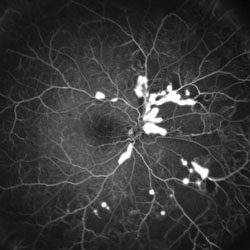
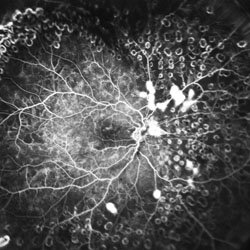
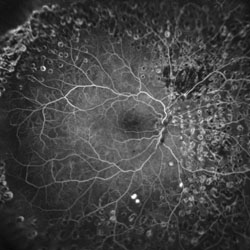
Dr. Singer says the idea is to reduce the production of VEGF in the ischemic part of the retina. “Think of it as watering the grass, and you’ve got a knot in the hose,” he says. “The water runs out after a while, and because the flowers don’t get any water they scream for help, putting out VEGF. That either builds more vessels, as happens in diabetes or severe ischemic CRVO, or increases inflammation, which causes macular edema. The idea is to stop the cycle by decreasing the amount of VEGF that’s produced. We’re pulling the flowers that are wilting out of the ground. Hopefully, by using targeted laser you won’t need to destroy much peripheral vision to stop the cycle of rebound macular edema.”
Dr. Singer says he’s only at the first stage of proving that this works. “The next stage will be to laser individuals for whom I already have wide-field maps,” he explains. “Then I can get quantitative data, hopefully showing that the cycle length between injections is longer, or that they don’t need any more shots.”
Dr. Brown is pursuing the same kind of approach. “If we know that the edema is triggered by VEGF, why not try to shut down the VEGF drive?” he asks. “Would peripheral laser to ischemic areas decrease the need for ongoing injections? That idea certainly makes sense, although it’s never been proven. Laser is inflammatory, after all, so a panretinal photocoagulation could trigger rebound edema.
“We’re currently doing two investigator-sponsored trials looking at peripheral laser ablation combined with anti-VEGF treatment,” he continues. “Half the patients are being randomized to Lucentis and half to Lucentis-plus-laser, using widefield Optos imaging. Hopefully we’ll get some preliminary data which will then guide a larger trial.”
The Decision Tree
Drs. Brown, Singer and Patel explain how they choose the best approach to use when faced with a new patient in the clinic. “When a patient comes in, if he’s relatively asymptomatic and functioning fine, I say, ‘We could treat you right away and maybe make this better, but the problem may fix itself,’ ” says Dr. Brown. “So, I give those patients four to six weeks to get better on their own. On the other hand, if a patient comes in and says, ‘I can’t see, I can’t drive,’ I typically inject anti-VEGF that day or within a few days to get some rapid relief.
|
“If a patient has a branch retinal vein occlusion with microaneurysms that are leaking, or areas of ischemia, I’ll discuss the possibility of doing adjuvant grid laser at three or four months,” he adds. “I’d typically do the treatment a week or two after the injection. If the patient has a central retinal vein occlusion, we talk about steroids vs. anti-VEGF, and how steroids may get you a little bit longer time between treatments, as well as the risk/benefit ratio. I also mention the possibility of peripheral laser, although at this point, I’m mainly only doing this in the confines of our randomized controlled trial.”
Dr. Patel notes that when dealing with macular edema secondary to retinal vein occlusion, every patient presents as a different therapeutic challenge. “Steroids and anti-VEGF are not mutually exclusive in patients with CRVO or BRVO, but choices must be made based on relative benefit/risk ratios as to which option will be the first-line treatment and which will take an adjunctive role,” he says. “That choice is always difficult.
“When patients come into the office with a retinal vein occlusion, the first thing I consider is their age,” he continues. “If they’re younger, I‘m concerned about a systemic abnormality—whether they have an underlying cardiovascular or hematological abnormality that may make them more prone to having retinal vein occlusion. Oftentimes, younger patients who present with retinal vein occlusion are not aware of having any systemic abnormality.
“This subset of patients must be diagnosed and treated aggressively, both locally and systemically,” he notes. “In atypical cases, such as younger patients and bilateral or recurrent retinal vein occlusions, I collaborate closely with my patient’s primary care physician. In the past, I’ve seen laboratory tests—such as a complete blood count, fasting serum glucose, serum protein electrophoresis, homocystein, serum viscosity or thrombophilic screening (factor V Leiden mutation, protein C or S deficiency, antithrombin III deficiency or antiphospholipid antibodies)—ordered with successful screening outcomes.
“The second thing I consider is the duration of the problem,” he continues. “Has the patient come in relatively soon after his vision has dropped, or did he wait? Patients who present right away respond well to either anti-VEGF or steroid treatment.
“I had a patient about a year and a half ago, just after Ozurdex was approved by the FDA, who came in with extensive macular edema the day after her CRVO,” he recalls. “Her vision in the affected eye was 20/400. We had a lengthy discussion about the pros and cons of treating with Lucentis vs. Ozurdex. She was in favor of Ozurdex because of the decreased treatment burden. It turned out that she only required one Ozurdex treatment and one grid laser treatment two weeks later. Her vision today is 20/25. Her outcome was amazing—she was one of those home-run patients.”
Regarding how long the problem has existed at first presentation, Dr. Brown notes that the BRAVO, CRUISE and COPERNICUS data showed that even patients who have six months or longer duration of blockage before they’re treated do benefit from therapy. “They gain quite a bit of vision, although they don’t seem to gain quite as much as those who start treatment early on,” he says. “In fact, I’m just as aggressive in treating someone who shows up with a six-month history as I am with somebody that shows up with a two day history—maybe even more so. The natural history studies suggest that about a third of those who have just suffered a blockage will improve on their own. The ones who’ve had the problem for six months are not going to improve on their own. If you don’t intervene with those patients, you’re only going to lose more ground.”
Dr. Patel says that when using anti-VEGF injections, his usual algorithm is treating the patient for the first six months with monthly injections. “There are two reasons I do this,” he explains. “First, it helps to clear the macular edema very quickly; within the first five days the patient notices a significant improvement in his vision, and the central macular thickness from the macular edema is halved—in some cases improved by as much as 85 percent. So you get a dramatic treatment effect. Second, it helps to rapidly clear the retinal hemorrhages that occur.”
Dr. Patel notes that these patients usually like to be seen regularly, and seeing them every month or every two to three weeks makes the rapport between the physician and patient much stronger. “These patients are usually very keen on getting some treatment and making sure that their vision is improving,” he says. “Coming in every month can be a burden for some patients and their families, but younger patients are generally all for it.
“After six months it’s best to continue monthly follow-up visits, and ranibizumab injections for recurrent edema have been shown to maintain visual benefit,” he adds. “If I find some minor residual edema in a BRVO patient after six months of anti-VEGF treatment, I’ll perform a grid laser therapy in the area of the macular edema. Combination therapy with grid laser, in my experience, has prolonged the therapeutic effect of the previous six months of injections.”
Dr. Patel notes several circumstances in which he’d be inclined to opt for Ozurdex rather than anti-VEGF drugs:
• When the patient has had a vitrectomy. “These patients do not have the vitreous sink to hold onto the anti-VEGF agent,” he says. “So if they have no IOP or glaucoma issues, I inject them with Ozurdex almost 100 percent of the time. Ozurdex provides stable drug levels in vitrectomized eyes, as opposed to the rapid clearance seen with Lucentis.”
• If the patient has an extensive cardiovascular history. “In this situation, steroids may be safer than anti-VEGF,” he notes. “I try to avoid using monthly anti-VEGF treatments, because these drugs do have a very small risk of systemic side effects.”
• If the patient has significant macular ischemia. “Suppose a patient has had diabetes before, and on top of the diabetes he develops a retinal vein occlusion,” says Dr. Patel. “Repeated anti-VEGF injections have been shown to increase macular ischemia. So in those patients you have to be very careful about giving frequent anti-VEGF injections.”
• If a treatment burden exists for the patient. In this type of situation I generally opt for treating with Ozurdex, which provides sustained release for up to six months.” he says.
What’s Next?
Dr. Singer acknowledges that none of these treatments really solves the underlying problem—the occlusion. “I believe that by giving all of these interventions we’re actually prolonging the disease course,” he says. “But hopefully we’re decreasing the amount of scarring and fibrosis and atrophy centrally that you’ll get compared to letting the body handle the problem on its own.
“To me, the question is not whether you can control the edema,” he adds. “The question is, can you stop the cycle? I’d like to see us reach a point at which we can eliminate the edema, leave the patient with good vision and have that improved vision last, within a year. I think this will come from a combination of an anti-inflammatory, an anti-VEGF and probably laser, timed at intervals.”
Drs. Singer and Patel anticipate eventually having the ability to deliver multiple drugs through a sustained-delivery platform. “In every other field of medicine, people use combination therapy,” notes Dr. Singer. “The way I see the future is, you find a sustained-delivery method, you put a number of different classes of drugs in it, and you give the patient a shot every six months. You mitigate the side effects and actualize the potential of the combination.”
Dr. Patel agrees. “Hopefully,” he says, “the next advance will be combination therapy with multiple drugs in an extended-release device, so the patient’s treatment burden is significantly reduced.”
Drs. Singer and Brown have been consultants to Genentech, Regeneron and Allergan, and have received research funding from all three companies. Dr. Patel has no financial ties to any company or product mentioned.