Clinching the Diagnosis
Physicians say that you increase your chances of saving the cornea by catching the fungus early and hitting it hard with medications. Here are their tips:
• Watch for the risk factors. “A major risk factor is where the clinician practices and where the patient lives or has visited recently,” says Francis Mah, MD, a corneal specialist at the Scripps Clinic in La Jolla, Calif. “Fungal infections, and fungal keratitis specifically, are a lot more common in hot, humid areas. If an ulcer patient says he has recently traveled to Singapore, for example, that should raise your suspicion of a fungal cause since that could be the region where it started. The second factor to be aware of is the history. Specifically, agricultural causes, or causes involving trauma from a plant, will be a common factor. Also, contact lens use or misuse can be a frequent factor.”
|
An unstable ocular surface can also pave the way for a fungal infection. “The other clinical setting to be wary of involves corneas in which ocular disease is chronic, with altered sensation contributing to an unhealthy ocular surface that can promote infection by a yeast, notably Candida, or other fungi,” avers Terrence O’Brien, MD, professor of ophthalmology at the Bascom Palmer Eye Institute, University of Miami Miller School of Medicine. “We’ve also observed fungal keratitis after LASIK with creation of a flap and associated dennervation, as well as after corneal transplant in which the patient’s corneal nerves are compromised, there is foreign material present in the form of sutures and there’s a concomitant use of a topical corticosteroid.”
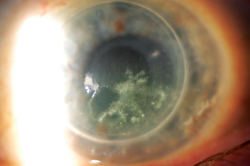
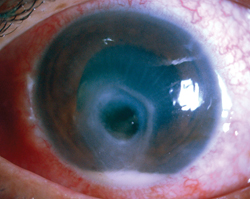
• Fungal features. Physicians say there are some features of fungal infections that stand out. “With bacteria, and even with Acanthamoeba, it’s a really acute process,” says Dr. Mah. “The eye will be normal one day and then painful with significant inflammation the next. Fungi take time to grow, so if the patient says his condition has been building for weeks, that may raise your suspicion of fungus.
“With fungus, you’ll see satellite lesions,” Dr. Mah continues. “These are pinpoint areas of infection across the cornea. Then, the infection will reach out and tend to go deeper than bacteria usually go.” Physicians also say to be watchful for ulcers with feathery borders and which involve endothelial defects that come and go. In some cases, they say, the epithelium will actually be intact while the fungal ulcer grows beneath it. “Also,” says Dr. Hannush, “in fungal keratitis the eye is often much quieter than you’d expect with a bacterial infection. So if I see a dense infiltrate, feathery or not, with an intact epithelium—or even without an intact epithelium—with a relatively quiet eye, I think atypical keratitis first, i.e., non-bacterial, specifically fungus.”
Cultures, Stains and Tests
Corneal specialists say that, to make a definitive diagnosis before initiating treatment, tests are mandatory.
• Stains. For a possible quick confirmation, stains are an option. “Gram stain, specifically KOH stain, is what I do specifically for fungus, especially when I’m not certain what the microbe is,” says Colleen Halfpenny, MD, assistant professor of ophthalmology at Jefferson Medical College in Philadelphia. Dr. O’Brien adds that other diagnostic stains can be employed, as well. “Giemsa staining can be helpful to identify the hyphal fungal fragments,” he says. “Also, Gomori methenamine silver is a stain that aids visualization of the hyphal fragments, and calcofluor white can also be used to highlight the fungal cell wall.”
• Cultures. It is usually easy to get a specimen for culturing when the pathogen is a fungus, physicians say. “If the epithelium is intact, you will have to debride it first,” says Dr. Hannush. “And, you will have to scrape pretty aggressively. When you get a sample, the ideal culture medium is Sabouraud agar, but fungus will frequently grow on thioacrylate broth or blood agar.” Sabouraud agar is preferred because it contains an antibacterial agent, and thus promotes fungal growth.
There may also be instances of polymicrobial infection. “In such cases you need to plate material on multiple selective culture media, such as blood agar, chocolate agar, Sabouraud agar, brain-heart infusion/gentamicin and thiol broth,” says Dr. O’Brien.
Dr. Mah says the way you culture can affect the results. “You never want to culture the very center of an ulcer,” he says. “This is because usually all that’s left in the center is necrotic tissue and you don’t actually get that much of the organism. Instead, you want to culture the edges of the ulcer. Grab a little of the viable epithelium if you can and put that on the culture plate. Also, you don’t want to go to the base of the ulcer because if some melting has occurred you may cause a corneal perforation.”
In cases where the epithelium is intact, some clinicians say you can still obtain material for culture without debriding the top layer of the cornea. “If the surface is uninvolved but there are branching filamentous infiltrates deep into the cornea, one method involving passage of a sterile suture can be helpful,” says Dr. O’Brien. “One can pass an 8-0 silk suture through the cornea at the level of the suspected infiltrate. You can then carefully remove the suture, which has passed through the zone of suspicion and, using sterile scissors, cut pieces of it off to place directly on the culture media for submission to the microbiology laboratory.”
• Biopsy. In some cases, corneal specialists say, the microbiological cultures will be inconclusive, and a biopsy can help make the diagnosis. Dr. O’Brien explains methods for performing a manual biopsy. “One can employ a single-use, sterile, dermatological skin punch of a specified diameter,” he says. “The punch is used to obtain material from the cornea and then submit it for microbiology, histopathology or even molecular microbiology with PCR testing. Other times, you can use a 0.12 forceps to grasp the edge of the infiltrate and then use a #11 Bard-Parker sterile, single-use blade to perform a shaving biopsy.”
Dr. O’Brien adds that, more recently, a femtosecond laser can be used to precisely, less-invasively and safely sample a specified area of the cornea for biopsy.
Treatment
The agent or agents used to eliminate the fungal ulcer depend on the variety of fungus you’re dealing with, experts say. The only commercially available agent is natamycin (Natacyn, Alcon), while the rest must be compounded. Here are tips for treatment.
• Medical therapy. “For an infection that’s non-filamentous or mostly yeast, which is most commonly Candida, my treatment of choice would be topical amphotericin 0.15%, which most compounding pharmacies can prepare,” says Dr. Halfpenny. “Topical capsofungin 0.5% can also be prepared at certain compounding pharmacies if there is too much toxicity from the amphotericin. Capsofungin is more expensive and harder to get, however.”
|
“For filamentous fungus, my treatment of choice would be topical natamycin 5% or topical voriconazole 1%,” says Dr. Halfpenny. “However, since the MUTT results were published, I tend to start with topical natamycin. For both filamentous and non-filamentous, I typically prescribe the drops to be used hourly around the clock for the first week, and then every two hours after that, depending on the patient’s response. It often may take several weeks to see clinical improvement, so I’m not quick to taper unless there is significant toxicity from the drops.”
One issue with treatment of fungal ulcers is the epithelium, since it can be intact in may cases. “Neither natamycin nor amphotericin penetrates the cornea well,” says Dr. Halfpenny. “So, if the epithelium is pretty well healed when you see the patient but he has grown out fungus, I’ll typically scrape the overlying epithelium before treatment. If he has an epithelial defect, though, I won’t scrape.”
The other treatment challenge is that fungal ulcers are often deep, and may need a two-pronged approach to treatment. “I will commonly start all patients with deeper ulcers on 400 mg oral voriconazole b.i.d.,” says Dr. Halfpenny. “However, they need to have liver function tests at baseline and be monitored again every two weeks.”
Finally, for very deep ulcers, some physicians use an intrastromal antifungal injection. “If the infection is very deep and you don’t think you’re getting good topical penetration, you can give intrastromal voriconazole,” says Dr. Halfpenny. “This has been shown to be safe, but not much more effective than topical voriconazole in very small studies.” Corneal experts say that, in general, they avoid the use of steroids in fungal ulcer management, as they’ve been shown to inhibit the effectiveness of antifungal therapy.
Clinicians say following the patient on therapy is as intense as the therapy itself. “One of the dictums with therapy is that it may get worse before it actually gets better,” says Dr. O’Brien. “This is because as treatment begins to kill the fungi, there’s a greater inflammatory reaction in the cornea. This is actually a sign of some improvement—it’s just more inflamed but you’re not seeing spread of the fungus. Positive signs of clinical response are a consolidation of the infiltrate, no sign of contiguous spread and the control of the satellite lesions.”
Clinicians say they’ll follow the patients daily or every other day while they’re on hourly treatment, spreading out the visits to weekly or every other week if the ulcer responds to treatment and begins to consolidate. The treatment could last for months.
• Therapeutic graft. Despite the ophthalmologist’s best efforts, medical treatment fails in 15 to 36 percent of cases.2,3 When this occurs, a therapeutic keratoplasty is necessary. For the corneal specialist undertaking one of these grafts, here are the experts’ tips.
When approaching the graft, Dr. Halfpenny has several considerations that she keeps in mind. “Try to keep the graft as small as possible, because it’s likely that you’ll need a secondary optical graft later, and you don’t want that area to become vascularized and not allow the secondary graft,” she says. “You should provide at least a 1- to 1.5-mm clear margin with the trephination, and be prepared to decenter the graft, if necessary. Also, you want to leave the patient phakic, even if he has the beginnings of a cataract, in order to leave a barrier to further fungal penetration or endophthalmitis. Postop, continue the oral or topical antifungal therapy and avoid topical or oral steroids for at least two to three days. You also should aggressively manage intraocular pressure with medications in the postop period because fungi have been known to destroy trabecular meshwork tissue. In light of this, the patient may need to see a glaucoma specialist or even require a secondary glaucoma surgery postop.”
With the daunting course an ocular fungal infection poses as a global threat to corneal health, Dr. O’Brien hopes significant advances in the field will be made soon. “We’re in desperate need of better antifungal agents that work more rapidly, penetrate more efficiently into ocular tissues and have fewer medical failures,” he says. “We have to both discover and develop newer compounds with novel mechanisms of action, greater antifungal activity and less cytotoxicity.” REVIEW
1. Prajna NV, Krishnan T, Mascarenhas J, et al. The mycotic ulcer treatment trial: A randomized trial comparing natamycin vs. voriconazole. JAMA Ophthalmol 2013;131:4:422-29.
2. Anane S, Ben Ayed N, Malek I, et al. Keratomycosis in the area of Tunis: Epidemiological data, diagnostic and therapeutic modalities [article in French]. Ann Biol Clin (Paris) 2010;68:4:441-47.
3. Prajna NV, Mascarenhas J, Krishnan T, et al. Comparison of natamycin and voriconazole for the treatment of fungal keratitis. Arch Ophthalmol 2010;128:6:672-78.


