Therapeutic soft contact lenses were first approved in the 1970s in the United States and have been used extensively to protect the cornea, relieve pain and enhance healing of the corneal surface. The variety of available materials and parameters has progressively expanded and has taken a large step forward with the arrival of the high-Dk silicone-hydrogel lenses.1-6 At the present time the armamentarium of therapeutic contact lenses allows the clinician to select lenses that will not only protect the corneal surface, but also modulate the healing process.1
This review summarizes the available contact lenses, the conditions most amenable to treatment, and the decision-making process that permits optimal selection of a therapeutic contact lens for a specific patient. Most of the hydrophilic soft contact lenses used for cosmetic correction are not approved for therapeutic use, but can behave well when used in an off-label manner as therapeutic lenses. It is important to communicate with the patient, when recommending use of a therapeutic contact lens, the goals of therapy, risks contingent upon contact lens use, and whether the lens is being used in an off-label fashion.
Available Therapeutic Contact Lenses
The water content, polymer chemistry, and lens thickness determine the oxygen permeability of the contact lens.7 The ionic character of the surface determines compatibility with topical medications and lens cleaners, and the likelihood of protein or lipid deposit formation.8,9 The design characteristics of the lenses also determine potential tear exchange on blinking and how likely the lens is to bind or crimp onto the cornea.
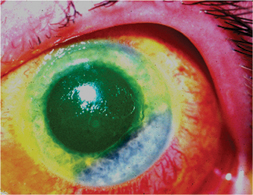 |
| A therapeutic lens may relieve painful bullous keratopathy. |
Therapeutic contact lens wear can be a long-term therapy, so chronic edema and corneal vascularization can be a consequence of such lenses. Although this outcome is usually considered a limitation to cosmetic wear, it can be a desired outcome when the clinician wants to induce vascularization into a peripheral melting lesion that has been applied with cyanoacrylate adhesive or when a peripheral lamellar patch graft requires rapid healing. Although the high-Dk silicone-hydrogel lenses have received recent approval for therapeutic use, they are not yet approved in the United States for therapeutic wear. Nevertheless, the performance profile of these lenses argues strongly for their potential value as a therapeutic choice, particularly when avoidance of corneal vascularization is a goal of therapy.10-14 While most lenses have similar diameters in the 13-15 mm range, some specialty therapeutic lenses (Kontur, Richmond, Calif.) have much larger diameters to facilitate coverage of the paralimbal region and the adjacent conjunctiva. Table 1 summarizes the available lenses and their characteristics of polymer chemistry, water content, diameter, Dk, and whether they have been approved by the Food and Drug Administration for therapeutic use.
Therapeutic Bandage Contact Lens
Broadly speaking, the indications for therapeutic contact lens include painful bullous keratopathy (corneal edema), corneal epithelial defects, corneal epithelial irregularity, corneal ulcerations, and as an adjunct to surgical care.15,16
Chronic corneal edema due to endothelial failure results ultimately in bullous epithelial lesions that break down and cause pain and irritation. Bandage contact lens therapy relieves pain but doesn't usually improve vision. A goal in therapy is to control pain while preventing corneal vascularization, particularly if the patient is a candidate for keratoplasty.
Epithelial Defects
• Recurrent corneal erosions. There are several different conditions that may cause recurrent corneal erosions. Anterior causes include abrasive trauma, epithelial basement membrane dystrophy, and Reis-Bückler's dystrophy. Stromal dystrophies such as granular and lattice dystrophy may also produce secondary corneal epitheliopathy.
Recurrent corneal erosions usually manifest with blurred vision, photophobia, pain and discomfort and are accompanied by slit lamp findings of focal epithelial edema, epithelial microcysts and loose epithelial attachments. The common pathophysiology of this disorder is an abnormal epithelial basement membrane adhesion complex, focal basal epithelial edema, and abnormal epithelial turnover.
• Persistent epithelial defects and ulcers. Bandage contact lenses are occasionally used in the management of persistent corneal epithelial defects and corneal ulcers, including post-infectious, trophic and autoimmune-related ulcers.
Soft contact lenses are sometimes utilized when treating infectious corneal ulcers to provide protection of the fragile, healing corneal epithelium while maintaining effective delivery of antibiotics via a depot mechanism.17-19
A trophic corneal ulcer usually presents as a persistent epithelial defect with possible stromal ulceration and is often associated with decreased corneal sensation. The goal in treating this lesion is to promote epithelial healing and prevent the secondary stromal ulceration. A soft contact lens with good oxygen permeability may provide protection of the healing epithelium.
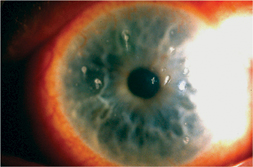 |
| Therapeutic contact lenses are benefical in cases of corneal epithelial defect from causes such as chemical/thermal burn, persistent epithelial defect, recurrent corneal erosion, and filamentary keratopathy. |
• Corneal irregularity. Bandage contact lenses can provide significant pain relief in conditions where the anterior surface of the cornea is elevated and irregular, sometimes even improving visual acuity. One such condition is filamentary keratitis, a disorder of irregular epithelial healing leading to mucous filament adhesion to focal epithelial micro-erosions of the cornea. Contacts lenses in this condition provide comfort and sometimes improve vision.
Contact lenses have also been reported to alleviate discomfort associated with other surface disorders such as Thygeson's superficial punctate keratitis and superior limbic keratitis (SLK).15,16
Postoperative Care
Bandage contacts lenses can be an extremely valuable adjunct when treating post-surgical conditions of the cornea and ocular surface. They aid in epithelial healing after planned surgical removal of the epithelium for procedures such as epithelial basement membrane disease, anterior corneal scar removal, phototherapeutic keratectomy, photorefractive keratectomy and LASEK.20,21 A bandage lens will protect the healing epithelium and provide significant pain relief in the postoperative period.
Bandage lenses can also be used for treating epithelial defects after penetrating keratoplasty, iatrogenic epithelial defects from a microkeratome pass during LASIK surgery, and after using cyanoacrylate adhesive for corneal perforations.
Bandage lenses have also successfully been used to manage bleb-related complications after glaucoma surgery. A bandage lens can be used to seal bleb leaks, to decrease bleb enlargement in cases of hypotony and to prevent pain from conjunctival suture abrasive trauma to the eyelids.22
Contraindications
The two contraindications for use of a contact lens are corneal anesthesia and extensive exposure with inadequate eyelid position or movement. If significant decrease in corneal touch sensitivity is present, the eye does not tolerate the contact lens and can develop significant inflammation. Small degrees of impairment of corneal sensation may permit use of a therapeutic contact lens, but the patient must be followed extremely closely to detect intolerance or complications at early onset.
Another relative contraindication is significant lagophthalmos or lid position abnormality. Localized drying of the contact lens causes mechanical irritation and abrasion to the surface of the eye as well as significant discomfort.
In conditions where a therapeutic lens is left in place for an extended period of time, it is best to remove the lens periodically and clean it to avoid protein and microbial buildup. While there is a report of prolonged wear of the same therapeutic contact lens for over 12 years. it is more prudent to replace the therapeutic contact lens periodically.23
Complications with Lens Wear
Contact lenses can alter corneal anatomy and physiology. Low-Dk hydrogel lenses can create significant hypoxia, hypercapnia and tissue acidosis for the cornea.24,25 Surface epithelial changes include edema, microcyst formation, decreased sensation, changes in junctional adherence between cells, and pannus formation.
There have been reports of stromal and endothelial complications with long-term contact lens wear.25 Lenses may induce hypoxia that induces superficial and stromal neovascularization. The majority of the changes in the cornea may be preventable and reversible with the cessation of long-term wear or with use of the high-Dk lenses.
Contact lenses have the potential to create significant ocular complications due to infection. Ocular surface infections are the most feared and significant complication of contact lens use. Corneal ulcers are seen with soft contact lens use and abuse.26-29 The risk of bacterial microbial keratitis can vary with the type and duration of wear of the lens.
Patient factors such as hygiene, smoking and overnight wear can add to the overall risk of infections.28 Pathogens such as Acanthamoeba, Pseudomonas, Serratia and other gram-negative bacteria in particular are very capable of adhering to contact lenses and causing bacterial keratitis. Others have also shown that particular lens types such as low-Dk and extended wear lenses may be associated with higher rates of infections.30,31
Papillary conjunctivitis and associated allergic inflammation of the ocular surface can be seen with therapeutic contact lens use.32 Studies have shown inflammatory mediators in the tear film of contact lens wearers, and, since tear clearance is also reduced in lens wearers, the inflammatory effect is increased.33
Peripheral corneal infiltrates can also occur in contact lens wearers and are more common in patients wearing extended wear soft contact lenses.34,35 While most infiltrates are sterile inflammatory reactions, some are probably due to low levels of less virulent pathogens.35
Severe intraocular inflammation rarely has been reported with contact lens wear and can include anterior chamber flare and cellular reaction, particularly in patients with significant decrease in corneal touch sensitivity or prior recurrent inflammation. Typically such complication occurs with a lens that is too steeply fit, producing a sucked-on-lens syndrome.16
Selecting an Appropriate Lens
If protection of the corneal surface is the only goal of contact lens therapy, then epithelial and stromal edema is best avoided. A high-Dk silicone hydrogel (balafilcon a, lotrafilcon a) or a very thin membrane-type lens (crofilcon) is the optimal choice. If the goal is not only surface protection but stimulation of stromal wound vascularization, then selection of a low water content, thick, hydrophilic lens (Plano T) is the better option. If the patient is prone to lens loss or requires frequent replacement of the therapeutic lens, then an economical selection is a daily disposable moderate water content lens.21,36
Certain circumstances recommend specific therapeutic contact lenses. Patients with a prior history of active giant papillary conjunctivitis may better tolerate a crofilcon glycerylmethacrylate lens, which has a lower incidence of GPC.
The advances in contact lens technology offer new options for the use of therapeutic contact lenses. With the new generation of high-Dk lenses potentially promising fewer problems of vascularization and infection, we are likely to see an increased use of these lenses in therapy.37-39 Nevertheless, the more traditional therapeutic contact lenses still offer useful options when considering the healing objectives of the particular treatment plan for a specific patient.
Dr. Foulks is a professor of Ophthalmology at the University of Pittsburgh where he is director of the cornea service and director of clinical research in the Department of Ophthalmology. He is past president of CLAO and chairman of the Board of Trustees of the CLAO Education and Research Foundation. Contact him at 412-647-2206.
1. Shah C, Sundar Raj CV, Foulks GN: The evolution in therapeutic contact lenses. Ophthalmol Clin North Amer 2003;16.
2. Dohlman CH: Complications in therapeutic soft lens wear. Tran Am Acad Ophthamol Otolaryngol 1974;78:399-405.
3. Amos D. Use of soft bandage lenses in corneal disease. Am J Optom Physiol Opt 1975;52:524-533.
4.Bodner B: Selection of Therapeutic Lenses. In: Dabezies OH, ed. CLAO Guide to Basic Science and Clinical Practice, Vol II, Chapter 47, New York: Grune and Stratton, 1984.
5. Mobila, E, Dohlman, CH, and Holly F. A comparison of various soft contact lenses for therapeutic purposes. Contact Intraoc Lens Med. J 1977; 3:9-15.
6. Lindahl K, DePaolis M, Aquavella J, Application of hydrophilic disposable contact lenses as therapeutic bandages. CLAO J 1991;17:241-243.
7. Oxygen permeability of the hypertransmissible contact lenses. Youn MD, Benjamin WJ. Eye and Contact Lens 2003;29:s17-21.
8. Bontempo AR, Rapp J. Protein and lipid deposition onto hydrophilic contact lenses in vivo. CLAO J 2001;27:75-80.
9. Jones L, Senchyna M, Glasier MA, Schickler J, Forbes I, Louie D, May C. Lysozyme and lipid deposition on silicone hydrogel contact lens materials. Eye and Contact Lens 2003;29:s75-79.
10. Brennan NA, Coles CC, Constock TL, Levy B: A one year prospective trial of balafilcon A PureVision silicone-hydrogel contact lenses used on a 30 day continuous wear schedule. Ophthalmology 2002;109:1172-1177.
11. Nilsson SEG. Seven-day extended wear and 30 day continuous wear of high oxygen transmissibility of soft silicone hydrogel contact lenses: a randomized 1 year study of 504 patients. CLAO J 2001;27:125-136.
12. Sweeney DF, Keay L, Jalbert I, Holden BA. Clinical performance of silicone hydrogel lenses. In: Silicone Hydrogels: The Rebirth of Continuous Wear. D.F.Sweeney ed. Oxford, England, Butterworth Heinemann, 2000, pp90-149.
13. Lim L, Tan DT, Chan WK: Therapeutic use of Bausch & Lomb PureVision contact lenses. CLAO J 2001;27:179-85.
14. Montero J, Sparholt J, Mely R. Retrospective case series of therapeutic applications of a lotrafilcon a silicone hydrogel soft contact lens. Eye and Contact Lens 2003;29:s54-s56.
15. McDermott ML, Chandler JW. Therapeutic uses of contact lenses. Surv Ophthalmol 1989;33(5):381-394.
16. Plotnik RD, Mannis MJ, Schwab IR. Therapeutic Contact Lenses. Intl Ophth Clinics 1991;31(2):35-52
17. Matoba AY, McCulley JP. The effect of therapeutic soft contact lenses on antibiotic delivery to the cornea. Ophthalmology 1985; 92(1):97-99.
18. O'Brien TP, Sawusch MR, Dick JD, Hamburg TR, Gotsch JD. Use of collagen shields versus soft contact lenses to enhance penetration of topical tobramycin. J Cataract Refract Surg 1988 Sep;14(5):505-7.
19. Tian X, Iwatsu M, Sado K, Kanai A. Studies on the uptake and release of fluoroquinolones by disposable contact lenses. CLAO J 2001;27:216-220.
20. Lim-Bon-Siong R, Valluri S, Gordon ME, Pepose JS. Efficacy and safety of the Protek (Vifilcon A) therapeutic soft contact lens after photorefractive keratectomy. Amer Jour Ophthalmol 1998;125:169-176.
21. Arora R, Gupta S, Taneja M, Raina UK, Mehta DK. Disposable contact lenses in penetrating keratoplasty. CLAO J 2000;26:127-129.
22. Blok MD, Kok JH, van Mil C, Greve EL, Kijlstra A. Use of the megasoft bandage lens for treatment of complications after trabeculectomy. Am J Ophthalmol 1990;110:264-268.
23. Kokolakis S, Baltatzis S, Zafirakis P, Livir-Rallatos G, et al. Twelve years' continuous wear of the same therapeutic soft contact lens: a case report. European Journal Ophthalmol 1999;9:312-4.
24. Holden BA & Mertz GW. Critical oxygen level to avoid corneal edema for daily and extended wear contact lenses. Invest Ophthalmol Vis Sci,1984;25:1161-67.
25. White PF, Miller D. Complications of contact lenses: Physiological complications-corneal edema. Int Ophthalmol Clin 1981;21:3-12.
26. Brown SI, Bloomfield S, Pearce DB, Tragakis M. Infections with the therapeutic soft contact lens. Arch Ophthalmol 1974;91:275-77.
27. Nilsson S, Montana P. The annualized incidence of contact lens induced keratitis in Sweden and its relation to lens type and wear schedule: results of a three-month prospective study. CLAO J 1994;20:225-230.
28. Liesegang TJ. Contact lens-related microbial keratitis: Part I: Epidemiology. Cornea 1997;16(2):125-31.
29. Cheng KH, Leung SL,Hoekman HW, Beekhuis WH, Mulder PG, Geerards AJ, Kijlstra A. Incidence of contact-lens associated microbial keratitis and its related morbidity. Lancet 1999;354:181-185.
30. Schein OD, Buehler PO, Stamler JF, Verdier DD, Katz J. The impact of overnight wear on the risk of contact lens-associated ulcerative keratitis. Arch Ophthalmology 1994;112(2):186-90.
31. Schein OD,Glynn RJ, Poggio EC, Seddon JM, Kenyon KR. The relative risk of ulcerative keratitis among users of daily wear and extended wear soft contact lenses: A case control study. New Engl J Med 1989;321:773-778.
32. Donshik PC. Giant papillary conjunctivitis. Trans Am Ophthalmol Soc, 1994:92:687-744.
33. Chang SW, Chang CJ. Delayed tear clearance in contact lens associated papillary conjunctivitis. Curr Eye Res 2002;22(4):253-7.
34. Baum J, Dabezies OH. Pathogenesis and treatment of "sterile" midperipheral corneal infiltrates associated with soft contact lens use. Cornea 2000;19: 771-81.
35. Donshik PC, Suchecki JK, Ehlers WH. Peripheral corneal infiltrates associated with contact lens wear. Trans Am Ophthalmol Soc 1995;93:49-60.
36. Gruber E: Acuvue disposable contact lens as a therapeutic bandage. Ann Ophthalmol, 1991;23:446-7.
37. Imayasu M, Petroll Wm, Jester JV, Patel SK, Ohashi J, Cavanagh HD, et al. The relation between contact lens oxygen transmissibility and binding of Pseudomonas aeruginosa to the cornea after overnight wear. Ophthalmology 1994;101:371-388.
38. Nilsson SE. Bacterial keratitis and inflammatory corneal reactions: possible relations to contact lens oxygen transmissibility: the Harold A. Stein Lectureship 2001. CLAO J 2002; 28(2):62-5.
39. Ladage PM, Jester JV, Petroll WM, Bergmanson JPG, Cavanagh HD. Role of oxygen in corneal epithelial homeostasis during extended contact lens wear. Eye and Contact Lens 2003;29:s2-s6.



