IT"S EASY TO BELIEVE THAT WAVEfront-guided ablation is superior to standard ablation. After all, today"s wavefront-guided procedures have consistently produced better outcomes than traditional procedures--at least in the United States.
According to Jack Holladay, MD, MSEE, FACS, clinical professor of ophthalmology at Baylor College in Houston, however, the improvement in outcomes may be the result of three advances in technology that have nothing to do with customized wavefront. In fact, he says, these same advances can be made part of standard software at a much lower cost to doctor and patient, producing outcomes at least as good. (Dr. Holladay says this has already happened internationally, especially in Europe.)
"Three changes have been made to the software in wavefront-guided systems that haven"t been made to standard system software, at least in the United States," he says. "As a result, wavefront-guided ablations do three things standard ablations do not: They keep the cornea prolate, produce larger astigmatic corrections, and reduce the formation of central islands. I believe these three changes account for the improvement in performance seen in comparative studies."
In fact, Dr. Holladay says that the whole idea of correcting higher-order aberrations by ablating the cornea is fundamentally flawed. "The Food and Drug Administration won"t allow manufacturers to claim that these systems correct higher-order aberrations, because manufacturer"s studies for FDA approval haven"t provided any scientific evidence that they do."
 |
|
Jack T. Holladay, MD, MSEE, FACS |
|
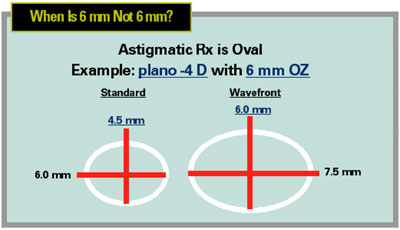
Houston surgeon Jack Holladay cites this example in which the wavefront treatment area is almost 25 percent larger than the standard treatment area based on the same prescription. |
Keeping the Cornea Prolate
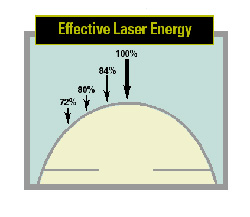
Laser ablations tend to produce an oblate cornea, says Dr. Holladay, because many of these lasers were first calibrated using a flat surface, not a dome-shaped surface like the cornea. "Any electromagnetic energy striking a surface, including excimer laser energy, becomes more spread out and less effective when the surface is tilted relative to the light source," he notes. "The laser"s effective energy drops off as the beam moves away from the center of the cornea, by 16 percent at 1 mm; 20 percent at 2 mm; and 28 percent at 3 mm. [See graphic, page 65.] This is the reason these lasers produce an oblate cornea; they"re not ablating as effectively away from the center of the cornea. All that"s necessary to correct this is to embed an energy compensation curve into the software."
Dr. Holladay says correcting this problem is important for two reasons. First, making the cornea oblate increases spherical aberration. "The surface of the cornea in front of the scotopic pupil must be prolate in order for the rays in the periphery not to bend too strongly, causing blurred focus," he says. "Making the cornea oblate increases the total spherical aberration of the eye, producing nighttime halos and glare complaints."
Second, an oblate ablation shrinks the optical zone. Three years ago, Dr. Holladay demonstrated that if you make the cornea more oblate, a greater optical correction produces a smaller functional optical zone.1 "For example," he says, "we did two -12 D treatments using the LaserSight laser. Our intention was to create a 6.5-mm optical zone. A standard treatment with the resulting oblate cornea produced an effective 5.5-mm optical zone. By doing nothing different for the second patient except compensating for the drop-off in energy toward the periphery, we produced an 8.5-mm optical zone." He has shown that a -5 D treatment without prolate compensation shrinks the optical zone by about 10 percent; a -10 D treatment shrinks it 25 percent.
Dr. Holladay adds that any excimer laser system can upgrade its software to make this correction and produce a prolate cornea. "With one exception—Wavelight"s Allegretto—laser manufacturers haven"t added this feature to their standard laser software in this country, only to their wavefront-guided software," he says. "Not surprisingly, the WaveLight Allegretto gets the best results of any standard laser ablation system in America today. Its results are equivalent to the wavefront-guided treatments of Visx, LADARVision and Technolas." 2 He notes that this feature is part of the standard software in Europe, and says that surgeons he has spoken with in Europe are favoring topography-customized ablations or standard prolate software instead of wavefront-guided systems.
"This prolate compensation is the major reason for the improved outcomes seen with wavefront-guided systems," he adds, "not customized wavefront measurements."
Sizing with the Smaller Axis
The second significant change made in wavefront-guided laser software, according to Dr. Holladay, involves the size of the astigmatic ablation zone. An astigmatic correction takes the form of an elliptical or oval shape which can be defined by two axes, one short (minor) and one long (major). Previously, when a laser was set to create a 6-mm optical zone, the software produced an astigmatic correction with a major axis that was 6 mm wide. This made the short axis less than 6 mm wide.
Dr. Holladay says a standard plano -4.00 x 90 degree treatment set for a 6-mm optical zone actually ends up being 4.5 by 6.0 mm. "About three years ago I explained to the FDA that when a 6.0 mm optical zone is specified it must be at least 6.0 mm in both the major and minor axes to be correct and avoid potential halos at night," he says. "They agreed, and as a result a plano -4.00 x 90 degree wavefront ablation is now 6.0 by 7.5 mm. This makes the wavefront treatment area almost 25 percent larger than the standard treatment area based on the same prescription.
"This means that when we compare overall results involving astigmatic correction done by wavefront-guided systems with results achieved using traditional system software, we"re comparing different size optical zones that are labeled as being the same! Is that a fair comparison? Absolutely not." He notes that a substantial number of patients in those comparative studies had astigmatism of 3 to 4 D, more than enough to have a profound impact on the resulting quality of vision.
Cleaning Up the Islands
The third change made in wavefront-guided systems is improved software designed to reduce islands in the center of the treated zone. Dr. Holladay says the specific change is proprietary and hasn"t been published by any of the companies, but like the other two improvements, in America this has only been incorporated into the software used in the wavefront-guided lasers.
He notes that several European laser systems currently provide all three upgrades as part of their standard laser package, including Carl Zeiss Meditec, Mel 80, Schwind and Wavelight. "However," he adds, "only Wavelight was willing to spend the time and money to get FDA approval to add these three features to its traditional laser system software in the United States."
A Problematic Premise
In spite of the improvement caused by the addition of these features, custom wavefront guidance leads to ablations that often increase higher-order aberrations, Dr. Holladay says. The exception: spherical aberration, which isn"t increased because the wavefront-guided systems keep the cornea prolate.
The reason, according to Dr. Holladay, is that most of the higher-order aberrations (excluding spherical aberration) are located in the crystalline lens; ablating the cornea won"t address that. To correct this is problematic if four ways:
- Correcting higher-order aberrations on the cornea creates an on-axis system. "The eye is a two-lens system," says Dr. Holladay. "Correcting a tiny bump on the crystalline lens with a tiny ablated divot on the cornea can only cause limited on-axis improvement for a single point at distance, such as a star. Points that are just a little off-axis may actually be made worse. If you"re looking at a printed word, the center letter will be clear, but the letters further away will get progressively less clear.
|
Related Articles |