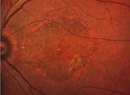
In a single-center, retrospective cohort study of 60 treatment-naïve central retinal vein occlusion patients, researchers sought to understand the relationship between baseline ischemic index (IsI) values calculated with ultra-widefield fluorescein angiography (UWFFA) and classification as an ischemic CRVO.
Researchers identified 60 eyes of 60 patients who were diagnosed with a CRVO between 2009 and 2016. The criteria for an ischemic CRVO included having an afferent pupillary defect and counting fingers vision or worse and/or neovascularization not attributable to another disease. Logistic regression was used to evaluate the relationship between IsI and the clinical outcomes.
The study found that patients with an IsI ≥35 percent were significantly more likely to become ischemic during the first year of follow-up than those with an IsI <35 percent (83.3 versus 13.9 percent, odds ratio 111, p<0.00001). In eyes with an IsI ≥35 percent, baseline and final logarithm of the minimum angle of resolution (logMAR) acuity were worse than those with IsI <35 percent (1.18 [a little better than 20/400] versus 0.46 [a little worse than 20/50], p<0.001 and 1.26 versus 0.45, p<0.001).
For eyes with IsI ≥35 percent, the researchers calculated a 50-percent probability of classification as ischemic CRVO in the one-year follow-up timeframe. The researchers also found that eyes with an IsI ≥35 percent were 100 times as likely to be classified as ischemic and six times as likely to have final acuity of 20/200 or worse in the first year of follow-up compared to eyes with an IsI <35 percent. Observed differences in vision were attributed in part to a greater prevalence of ischemic maculopathy and foveal avascular zone enlargement in eyes with an IsI ≥35 percent.
Retina 2019;39:6:1033-8.
Thomas AS, Thomas MK, Finn AP, Fekrat S.
Nailfold Capillary Blood Flow And Exfoliation Glaucoma
Researchers from New York, Boston and Chiang Mai, Thailand, say that, since analyzing patients’ blood flow using nailfold capillaroscopy has demonstrated alterations associated with high-tension glaucoma and normal-tension glaucoma, it’s possible that exfoliation glaucoma may also cause such changes. They undertook a study to try to find a connection.
The cross-sectional, clinic-based study was carried out at the New York Eye and Ear Infirmary of Mount Sinai from July 6, 2017, to May 18, 2018. The researchers studied 111 patients (30 XFG, 30 NTG, 30 HTG, and 21 controls). Exclusion criteria were the presence of connective tissue disease, uncontrolled diabetes, history of bleeding disorders, and/or history of trauma or surgery to the nondominant hand. The primary outcome was resting capillary blood flow at the nailfold of the fourth digit of the nondominant hand in patients with XFG, NTG, HTG and controls, using nailfold capillaroscopy.
Ultimately, two participants were exluded due to poor nailfold image quality, leaving 109 patients for the final analysis. Sixty-two participants (57 percent) were women and 79 (72 percent) were white. The average age of the participants was 67.9 ±11.7 years.
Mean resting peripheral capillary blood flow at the nailfold for controls was 70.9 ±52.4 picoliters/s (pL/s); HTG: 47.5 ±41.9 pL/s; NTG: 40.1 ±16.6 pL/s; and XFG: 30.6 ±20 pL/s. Multivariable analysis of the differences of flow in HTG vs control participants showed values of -18.97 (95% CI, -39.22 to 1.27; p=0.07) pL/s, NTG vs. controls of -25.17 (95% CI, -45.92 to -4.41; p=0.02) pL/s, and XFG vs. controls of -28.99 (95% CI, -51.35 to -6.63; p=0.01) pL/s.
The researchers say the study hints at the systemic nature of glaucoma, since the resting peripheral capillary blood flow decreased in patients with exfoliation and normal-tension glaucoma.
JAMA Ophthalmol 2019;137:6:618-625.
Kertes PJ, Galic IJ, Greve M, et al. FUS and the Rubella Virus-Associated Uveitis
FUS and Rubella Virus-Associated Uveitis
Researchers in the Netherlands sought to investigate and expand knowledge of ocular manifestations and complications of RV-associated uveitis and to demonstrate its relation to rubella vaccination and Fuchs uveitis syndrome.
A retrospective study of 144 eyes of 127 uveitis patients RV-positive in aqueous humor analysis was carried out. Patients were chosen from between January 2010 and October 2016. The average age at presentation was 37, and no cystoid macular edema was encountered preoperatively. None of the patients was vaccinated against RV. Uveitis was classified mainly as anterior uveitis or panuveitis, despite vitritis in 103 (81 percent) patients.
During the study, cataracts affected 67 percent of patients and five eyes presented with glaucoma at the end of follow-up. Thirty-nine patients presented with complete FUS phenotype, with 37 testing positive for RV (95 percent) and two patients (5 percent) testing negative. No alternative cause of uveitis was found in the two RV-negative FUS patients.
The researchers conclude that RV-associated uveitis and FUS aren’t exchangeable. RV-associated uveitis has a wider spectrum of clinical signs than typical features of FUS phenotype. This study supports the finding that FUS is mostly caused by RV in Europe. However, the researchers note that FUS has other causes such as CMV, T. gondii, and trauma, and not all RV-associated uveitis cases exhibit classical features of FUS. In this study, RV occurred in the aqueous humor of nearly all FUS patients, but RV presented as FUS only in a minority.
The researchers say that with correct diagnosis of RV-associated uveitis patients can avoid unnecessary immunosuppressive therapies and corticosteroids.
Am J Ophthalmol 2019;202:37-46
Groen-Hakan F, Van de Laar S, Van der Eijk-Baltissen A, Ten Dam-Van Loon N, De Boer J, Rothova A.
Survivor: Goldmann Tonometer
Because calibration error (CE) is one of the most common sources of error for Goldmann applanation tonometers, researchers implemented a preventative maintenance program for 190 tonometers to measure survival rates and report maintenance outcomes.
The prospective cohort study was carried out at two tertiary eye care referral centers on slit-lamp-mounted GATs (Model AT 900 C/M; Haag-Streit). The maintenance program consisted of monthly testing by ophthalmologists for one year. Reported repairs were fixed within 24 hours. Only CE at the clinically significant level of 20 mmHg was reported.
Acceptable CE level was deemed ±2 mmHg at all levels of testing. Instruments were considered faulty if the CE exceeded this limit at any testing level. Failure was defined as having developed an unacceptable CE beyond the third repair. The outcome measures included frequency of CE and the survival rate of the tonometer.
Sixty-three tonometers (33.1 percent) needed more than one repair. The remaining 127 instruments (66.8 percent) required no repairs. Of the GATs requiring repair, 49 (77.7 percent) needed one repair, five (7.9 percent) needed two repairs, two (3.1 percent) required three and seven (11.1 percent) developed unacceptable CE after the third repair and were removed from the program.
Among tonometers requiring one CE repair, the survival rate was 100 percent. For those requiring more than one repair, the survival rate was 0.64 after three months, dropping to 0.40 at the end of the study. The maintenance program didn’t halt the decline of units requiring maintenance, and the researchers reported that the number of repairs rather than the age of the unit determined survival. The researchers concluded that these monthly maintenance procedures can save time and money.
J Glaucoma 2019;28:6:507-11
Choudhari NS, Richhariya A, Wadke V, Deshmukh SP, George R, Senthil S, Sekhar GC.
Restrictive Strabismus After Pterygium Excision
Researchers from San Diego and the Tel Aviv, Israel, conducted a study to report characteristics of restrictive strabismus and diplopia development in patients following pterygium excision and approaches to treating postoperative restrictive strabismus.
The retrospective interventional case series was carried out at a single academic institution on 15 patients (mean age 49) who developed restrictive diplopia after pterygium excision. Inclusion criteria for diplopia on presentation was a history of ≥1 pterygium excision procedures before presentation of diplopia. Cases of diplopia due to other reasons were excluded.
The researchers report that all patients had an esotropia after excision of pterygium, which caused the diplopia. The mean time for diplopia onset after the last surgery was six months.
A combined procedure to remove scar tissue formation and improve diplopia was performed by a strabismologist and an oculoplastic surgeon. Amniotic membrane grafts secured with sutures rather than fibrin glue were used on all 15 patients. At 24 months of follow-up, only two patients required surgical intervention, which led the researchers to believe that securing AMGs with sutures was less inflammatory than glue, though no direct comparison was done.
Given the frequency of pterygium excision and AMG placement with glue, the researchers say that it’s important to be aware of the possibility of postoperative restrictive strabismus and its correction potential.
Am J Ophthalmol 2019;202:6-14
Baxter S, Nguyen B, Kinori M, Kikkawa D, Robbins SL, Granet DB.