In the fall of 2022, the European Society of Cataract and Refractive Surgeons debuted a new tool on its website that aggregates major online intraocular lens calculators into one site. Using the free online tool, surgeons can input their data once and then easily compare the results of up to seven calculators, including the Barrett Universal II, Cooke K6, EVO, Hill-RBF, Hoffer QST, Kane and Pearl DGS.
The idea originally came from Dante Luis Buosanti, MD, an ophthalmologist in Buenos Aires, Argentina. After reaching out to Kenneth J. Hoffer, MD, for permission to include his formula in the project, he and Dr. Hoffer approached ESCRS together to see whether the society would be interested in hosting this IOL calculation tool on its website. With the support of ESCRS board members, they secured permissions from the rest of the formula authors. The tool is available at iolcalculator.escrs.org.
How It Works
To create the calculator, the developers used a technique called web scraping, where bots extract information from other websites and bring it back to a single site. “Most of us are already familiar with web scraping to some degree,” says ESCRS president Oliver Findl, MD, MBA, FEBO. “When you go to Google or other search engines to book a flight, you enter where you want to fly and the dates and times, and Google searches all the different airlines and looks for flights that fit your criteria. All of that information comes back to Google, and you’re presented with your options, rather than having to go to each site individually and re-enter your information.”
 |
|
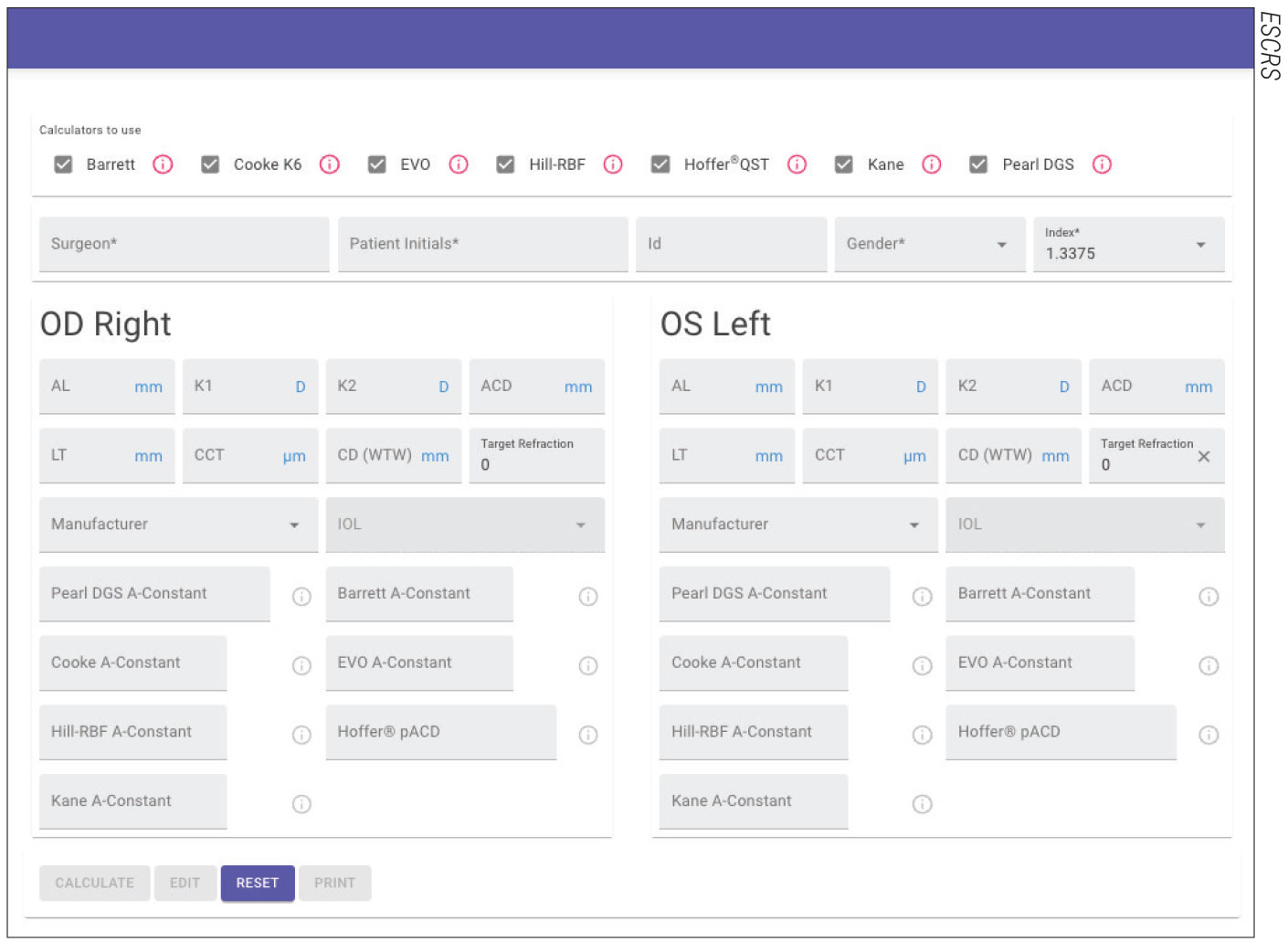
With the ESCRS calculator, surgeons can obtain results from seven different formulas by entering the patient data only once. Experts say this helps to save time and reduce data entry errors. |
Not only is it boring and time-consuming to enter data into each calculator manually, he adds, but data entry mistakes may also occur at some point. “The ESCRS IOL calculator requires much less work and reduces the potential for error because you only have to enter the biometry data once,” he says. “You receive a printout at the end with all of the formulae results next to each other. For example, it may say a 22-D lens of a certain manufacturer will have x predicted postoperative refraction for calculators one, two, three, four, etc. The more information we have the better.”
Since the tool uses web scraping, any updates or improvements to the original calculators on their respective websites will automatically be seen in the ESCRS calculator. The ESCRS calculator also has a list of optimized IOL constants from IOLCon (iolcon.org) that can be used depending on the user’s preference. “This ensures you’re always using the most current IOL constant for a lens,” Dr. Findl says. He adds, “We’re very grateful to the authors of these formulae to let us bring them together on the ESCRS platform.”
Strength in Numbers
Eduardo Viteri, MD, medical director of the Centro Oftalmológico HumanaVisión in Guayaquil, Ecuador, has tried the new ESCRS calculator in a few cases. He says the design is “elegant and user-friendly” with a report that’s easy to interpret.
“Most cataract surgeons already have a well-proven biometric protocol,” he says. “I usually calculate my cases with a Pentacam AXL, and the patients end up with a refraction close to the expected. What we want to avoid are refractive surprises that happen mostly in eyes that are on the extreme ranges of axial length or corneal curvature, or those with previous corneal surgery or pathology. Those are the cases where we’ll take the extra time and effort to use multiple formulas or calculators. However, in those outliers we may end up with IOL power suggestions with a range of 1.5 or more diopters, and the surgeon may reach a conclusion that the calculator is of little use. So, the reality is that the [ESCRS] calculator will be mostly used in cases with the worse predictability, whatever the calculator or formula.”
Having seven online calculators returning results helps with the informed consent process in these atypical cases, experts say. “If the calculators are in relative agreement with each other, we can tell the patient there’s a high probability that we’ll be really close to the refraction we’re aiming for,” Dr. Findl says. “If the results are all over the place, then we can inform the patient that their eye is difficult to calculate and that there’s a greater chance we may need to do some secondary procedure to correct the refractive surprise.”
Dr. Viteri agrees: “If the results are consistent among most of the formulas, I feel more confident that the postop result will be as expected. If I get dispersed results, I emphasize to the patient the high probability of a residual refractive error. In those cases, I usually choose an IOL on the myopic side of the average among calculated powers.”
He ran an informal poll in ophthalmologist groups asking, “Which of the ESCRS IOL calculator formulas do you think is more accurate?” and found that, “among more than 100 respondents, the formula they trust most is Barrett, followed by Kane as a far second. The rest of the formulas aren’t considered significantly better or more precise. I also found that as many as 40 percent of the responding surgeons haven’t tried the ESCRS calculator.”
Dr. Findl says a toric version of the ESCRS calculator is in the works with a tentative release date in the first quarter of this year. A post-refractive surgery calculator will be available in the summer of 2023.




