The American physician and signer of the Declaration of Independence Benjamin Rush once said, "Controversy is only dreaded by the advocates of error." If that's true, then he would be proud of refractive surgeons, since they don't shy away from a controversy. Each year at the meeting of the American Society of Cataract and Refractive Surgery,
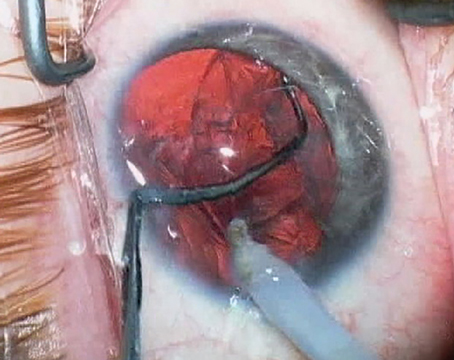
Refractive Surgery in Herpes Simplex
Though it's possible for the excimer to induce a recurrence of herpes simplex virus, some surgeons think refractive surgery is possible in select cases.
"I won't do it," says
A history of herpes keratitis is a relative contraindication for excimer surgery for some surgeons, but an absolute one for others.
Other surgeons, though, point to studies in which the risk of recurrence could be minimized.
"One of the challenges is we always want to do the best job for our patients while avoiding any issues," says
Louisville
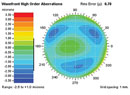
How Thin Is Too Thin?
With the specter of ectasia hovering over refractive surgery, more thought is being devoted to the thickness of the residual stromal bed in LASIK, and what the real risks for ectasia are.
Dr. Stonecipher says that a poll of the audience at the most recent controversies course showed that the residual stromal bed had crept up to 300 µm from the usual 250-µm cutoff. For his part, he says using the IntraLase has allowed him to make thinner flaps, increasing the residual stromal bed, and he has been able to leave a bed of 376 µm in more than 6,000 LASIK eyes at his practice.
Minneapolis
Lexington
Dr. Trattler tries to stay above the 250-µm residual bed limit, and says he "hopes to be in the 300 range in case the flap is thicker than expected," but puts more emphasis on corneal shape than thickness when trying to avoid ectasia. "For LASIK or PRK, I think shape is the most important risk factor," he says. "If the cornea is shaped normally but a little thin, there's no evidence that that causes ectasia." To cast doubt on the emphasis on thickness as a key risk factor, Dr. Trattler points to a study he performed in his practice of 94 eyes of 71 post-LASIK ectasia patients. Only 10 (11 percent) of the ectatic eyes had corneal thicknesses thinner than 500 µm preoperatively.
Dr. Trattler performs intraoperative pachymetry on every patient just to be sure he didn't get an inadvertently deep flap, and also because, he says, "that flap information is critical if we're ever going to understand post-LASIK ectasia."
Rheumatoid Arthritis Patients
Surgeons approach RA patients with caution, if at all.
"I look very carefully at these patients for controlled dry eye and no significant cataract," says Dr. Hardten. "This is because a lot of them have been on steroids in the past. I make sure that their systemic disease is well-controlled. Just like before cataract surgery in an RA patient, I put them on pre- and postop oral prednisone to try to help reduce the chances of immunologic melt. I published a paper about a patient with an immune melt.3 Anytime you operate on a patient with rheumatoid arthritis, there's the possibility of wound melting." He treats their dry eye with Restasis and sometimes punctal plugs.
Dr. Ferguson will operate on these eyes, but with conditions. "I'll do it if the systemic disease is under control, one eye at a time, separated by six weeks," he says. "They have to have gone three to six months without flare-ups and they should have a history of no ocular manifestations. If there have been any ocular manifestations of it, I'll avoid them. Even on a lens exchange, these limbuses can get so hot and pour out so much collagenase that they'll get a limbal melt."
Dr. Fowler avoids performing refractive surgery on any RA patient. "The idea of 'first, do no harm' is kind of the philosophy behind my approach," he says. "I've had to manage perforations, scleral melts and corneal melts in these patients after the fact, and it only takes your first one to start thinking that it's a real issue."
Dr. Stonecipher avoids certain patients, but doesn't rule out the procedure. "I look at their ocular surface disease," he says. "If they have OSD, I won't even think about it. If I do treat someone, though, I'm more prone to do so in the summer, because it's more humid and I think they heal better then."
1. Dhaliwal DK, Romanowski EG, Yates KA, et al. Experimental laser-assisted in situ keratomileusis induces the reactivation of latent herpes simplex virus. Am J Ophthalmol 2001;131:4:506-7.
2. Asbell PA. Valacyclovir for the prevention of recurrent herpes simplex virus eye disease after excimer laser photokeratectomy.
Trans Am Ophthalmol Soc 2000;98:285-303.
3. Lahners WJ,