A 56-year-old woman presented with nonspecific infero-nasal visual field loss in the right eye. The vision loss was noticed upon waking two weeks prior. She denied any pain, trauma, headache, diplopia, photophobia or infection.
Systemic review was significant for chronic hand numbness and pain secondary to rheumatoid arthritis, but was otherwise negative—she denied presence of any rashes, headache, jaw claudication, scalp tenderness, abnormal bowel movements or urinary symptoms.
Medical History
Medical history was significant for rheumatoid arthritis, for which she was on prednisone 5 mg and had stopped rituximab infusions nine months before. She also had a history of having had a positive purified protein derivative test for tuberculosis (PPD), which was treated with “months of antibiotics” two years prior to presentation. She also had hypertension and hypothyroidism. She denied tobacco use or drinking, denied illicit drug use and did not have any allergies.
Medications included: daily prednisone 5 mg; carvedilol 6.25 mg; ramipril 10 mg; armour thyroid 45 mg; and venlafaxine 75 mg. She had completed five courses of rituximab infusions occurring every six months over the past several years before stopping nine months prior to presentation due to insurance issues.
Examination
Examination demonstrated a best corrected visual acuity of 20/30 in the right eye without pinhole improvement and 20/20-2 in the left eye. External examination was within normal limits; no mass, proptosis or ptosis was noted. Pupillary exam was normal with no afferent pupillary defect. She was orthophoric in all positions of gaze and extraocular motility was full bilaterally. Confrontation visual fields disclosed an infero-nasal defect OD but were otherwise full to confrontation OU. Ishihara color plates were 15/15 OU.
Anterior slit-lamp examination of the right and left eyes were within normal limits—conjunctiva was quiet, cornea clear, anterior chamber quiet and lens clear. Intraocular pressure by Goldmann applanation tonometry was 16 mmHg OU.
Funduscopic examination of the right eye disclosed optic nerve head edema with trace vitreous white cells (See Figure 1). Funduscopic examination of the left eye showed a small crowded nerve without edema.
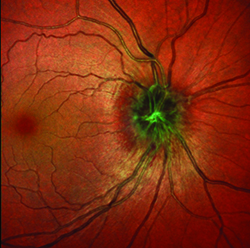 | 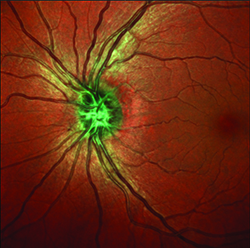 |
| Figure 1. Multicolor fundus optical coherence tomography demonstrating nerve head edema OD and crowded nerve OS. | |
What is your differential diagnosis? What further workup would you pursue?
Please click this link for diagnosis, workup, treatment and discussion.
Please click this link for diagnosis, workup, treatment and discussion.


