A 48-year-old African-American male presented with a two-month history of right upper lid swelling with recent-onset tearing and crusting of the eyelashes. He denied vision changes, diplopia, pain, history of trauma or recent illness. Systemic review of symptoms was negative for joint pain, shortness of breath, cough, abnormal bowel movements or urinary symptoms, but did reveal a recent rash on his upper and lower extremities for a week, with two days of facial skin involvement. He had initially presented to an outside hospital and had completed a course of oral cephalexin and topical bactroban without symptom resolution.
Medical History
The patient had no significant medical history, but did have a history of decreased color vision in both eyes. He denied tobacco, alcohol and intravenous drug abuse. He was not on any medications, and denied any known drug allergies.
Examination
The patient was afebrile with stable vital signs. His external examination demonstrated multiple crusted erythematous plaques on his face and neck. There was a soft, non-tender, mobile mass beneath the right upper lid with consequent mechanical and neurogenic right upper lid ptosis, demonstrated by decreased levator function. There was 2.5 mm of right hypoglobus. Hertel exophthalmometry revealed 5 mm of right-sided proptosis (See Figure 1). There was no eyelid erythema or tenderness and no resistance to retropulsion.
The best-corrected visual acuity was 20/20 OU. Pupillary exam showed no anisocoria or relative afferent pupillary defect. A left hypertropia was present in primary gaze, and extraocular motility revealed only 50 percent supraduction of the right eye with proportionately vertical binocular diplopia in upgaze. Visual fields were full to confrontation in both eyes. Ishihara color plates were 5/8 in both eyes, and the patient said this was normal for him.
Anterior slit-lamp examination and fundoscopic examination were unrevealing with no signs of inflammation or infection. Intraocular pressures were 17 mmHg OU by Goldmann tonometry.
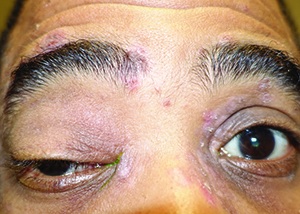 |
Figure 1. External photography demonstrating right orbital mass with associated ptosis, proptosis and hypoglobus, along with diffuse crusted, erythematous skin lesions.
|
Please click this link for diagnosis, workup, treatment and discussion.


