Presentation
A 68-year-old male presented to the Wills Eye Glaucoma Service with an elevated intraocular pressure in his left eye without any symptoms. He had previously undergone bilateral laser peripheral iridotomies and been diagnosed with mixed mechanism glaucoma in both eyes; he had undergone a trabeculectomy in the right eye. He had no history of ocular trauma, uveitis, infection with herpes simplex or zoster, or steroid use.
Medical History
There was no past medical history. The past ocular history included lattice corneal dystrophy and cataract surgery in the right eye, in addition to mixed mechanism glaucoma, as noted above. Current medications were latanoprost 0.005% nightly and timolol 0.5% two times a day, in the left eye only. He was intolerant to brimonidine, brinzolamide, dorzolamide and bimatoprost. Family and social histories were non-contributory.
Examination
On exam, visual acuity was 20/60 OD and 20/40 OS with no improvement on pinhole. Pupils and extraocular motility were normal. Intraocular pressures were 12 mmHg OD and 21 mmHg OS with central corneal thicknesses of 509 and
512 µm, respectively. The angle was open on gonioscopy with a Spaeth classification of C35f, with light trabecular meshwork pigmentation OU. Confrontation visual fields were normal. Slit lamp examination revealed a diffuse, slightly elevated, mildly vascular bleb and a posterior chamber intraocular lens OD, and a nuclear sclerotic cataract OS. On fundus examination, the optic nerves showed a cup-to-disc ratio of 0.8 and 0.7 OD and OS, respectively, with superior notching OU. The remainder of the fundus exam was unremarkable.
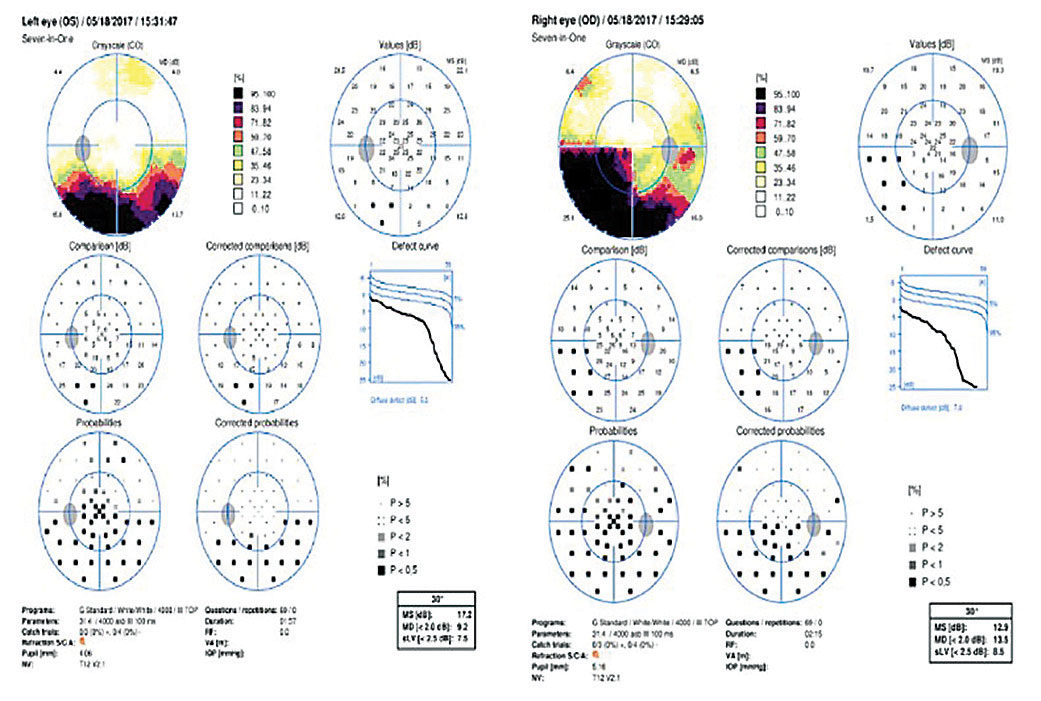 | 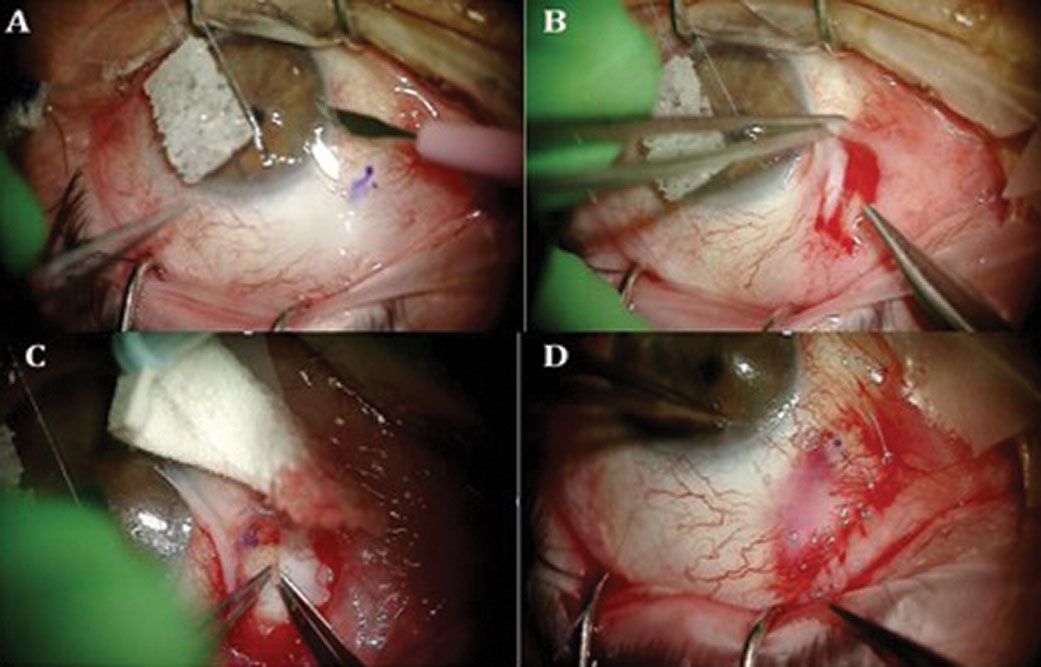 | |
| Figure 1. Octopus visual fields of the right and left eyes showing bilateral dense inferior arcuate defects. | Figure 2. Representative images from the reoperation to revise the fibrotic XEN Gel Stent. |
What is your diagnosis? What further workup would you pursue?
Please click this link for diagnosis, workup, treatment and discussion.


