A 55-year-old Caucasian female noted photophobia and blurred vision in both eyes. Her symptoms initially started three months prior to presentation with photophobia that spontaneously resolved. One month prior, she developed blurred vision associated with a head-to-toe rash, and ophthalmic evaluation revealed subretinal fluid and slight “retinal pigmentation” bilaterally. She was started on difluprednate drops four times a day, which reportedly decreased the subretinal fluid, and her visual acuity fluctuated. She presented to the Oncology Service of Wills Eye Hospital for a second opinion.
Medical History
Past medical history disclosed metastatic cutaneous malignant melanoma to the right hip from an unknown primary site one year prior to presentation. She underwent treatment with ipilimumab, pembrolizumab, and dabrafenib. Nine months following diagnosis, she was found to have brain metastases and underwent Gamma Knife radiotherapy. Additional medical history included bilateral mastectomy without need for chemotherapy, radiation or hormone therapy. The patient did not specify the reason for mastectomy, but there was a strong family history of breast cancer. In fact, there was family history of multiple family members with cancer (lung carcinoma, prostate carcinoma, breast carcinoma, cutaneous melanoma). Her social history was unremarkable.
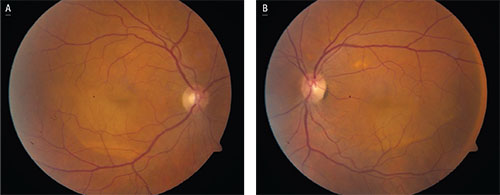 |
| Figure 1. Fundus photos of the right (A) and left (B) eyes demonstrating dependent vitelliform lesions associated with multifocal pockets of subretinal fluid. |
The patient’s current medications included: dabrafenib; pembrolizumab; difluprednate drops; prednisone (patient reported that she was taking it at varying doses and frequencies); temazepam and alprazolam. Her symptoms started while she was off dabrafenib.
Examination
Ocular examination demonstrated an uncorrected visual acuity of 20/50 OD (pinhole: no improvement) and 20/60 OS (PH: 20/50). Pupils were equal, round and reactive to light without relative afferent pupillary defect. The patient declined applanation, but intraocular pressure by finger tension was normal. Confrontation visual fields and extraocular motility were full bilaterally. The anterior segment examination was only remarkable for early nuclear sclerosis bilaterally.
Dilated fundus examination revealed shallow subretinal fluid in the macular region of both eyes, with smaller pockets of fluid in the extramacular region as well (See Fig. 1). Also present was bilateral subretinal vitelliform debris, which accumulated at the bottom of the subretinal fluid, producing a pseudohypopyon appearance.
Please click this link for diagnosis, workup, treatment and discussion.


