Diagnosis, Workup and Treatment
Differential diagnosis included inflammatory, infectious, neoplastic and traumatic causes. Brain and orbit MRI demonstrated left-sided reticulation of retrobulbar fat with enhancement of the pre-septal tissues, sclera and choroid. There was also mild enlargement with enhancement of the left lacrimal gland. The brain was normal. The patient had an elevated erythrocyte sedimentation rate (70) and C-reactive protein (3.3). Additional laboratory testing was unremarkable and included CBC; blood cultures; HLA B27; ACE; lysozyme; Toxoplasma antibodies; Toxocara antibodies; HSV antibodies; VZV antibodies; RPR, RF; FTA-Abs; cANCA; pANCA; chest radiograph; and urinalysis.
He was admitted with a working diagnosis of panuveitis and started on topical prednisolone acetate 1% every hour and atropine 1% twice daily. Skin testing for tuberculosis was negative at 48 hours, and he was started on a 1 mg/kg intravenous steroid pulse. He quickly felt better with vision improvement to hand motion. There was dramatic condensation of the fibrin disc in his anterior chamber. Intraocular pressure decreased to 6 mmHg. B-scan ultrasound showed dense vitreous debris with suprachoroidal collections of fluid or blood (See Figure 2). Diagnostic pars plana vitrectomy was planned as an outpatient. After three days of intravenous steroids, he was discharged home on 60 mg of oral prednisone daily. He also continued on topical prednisolone acetate 1% every hour while awake, loteprednol ointment at bedtime, and atropine 1% twice daily.
Two days later, he presented for follow-up with fevers, eye pain and malaise. We discovered that the patient was incorrectly taking only 20 mg of prednisone daily. His anterior segment exam had regressed to its initial appearance with new early neovascularization of the iris, and his intraocular pressure was now 46 mmHg. The patient underwent pars plana vitrectomy, which revealed purulent vitreous aspirate. He was given intravitreal vancomycin and ceftazidime and admitted for intravenous antibiotics. Vitreous cultures revealed heavy growth of methicillin-sensitive Staphylococcus aureus. Blood cultures, echocardiogram, dental examination and bone scan were normal.
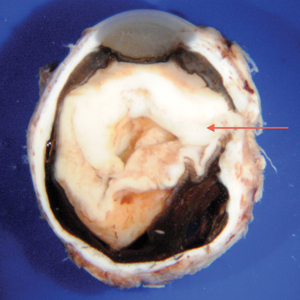
The infectious disease service was consulted and no systemic source for infection was identified. The patient’s condition continued to worsen. Four days after vitrectomy, the vision in the patient’s left eye was no light perception. He developed warmth and erythema of the eyelids and started to complain of pain with extraocular movements. MRI demonstrated two areas of globe rupture near the equator associated with contiguous orbital abscess (See Figure 3). Enucleation was performed. Gross and microscopic examination confirmed endophthalmitis secondary to Staphylococcus (See Figure 4).
|


Two weeks after enucleation, the patient and his mother disclosed that the step-father had been physically abusive to the patient. Although there had been several instances of head trauma, they remained confident that there was never any trauma involving the eyes.
Discussion
Infectious endophthalmitis is a rare and potentially devastating condition resulting from either the exogenous or endogenous spread of bacteria into the eye.1 Most commonly, this form of panuveitis presents with reduced vision, progressive vitritis and hypopyon, as well as substantial red eye, pain and lid swelling.2 Our patient had a remarkable absence of all of these signs except for the vitritis and reduced vision. Exogenous endophthalmitis is more commonly encountered and can occur following surgery, trauma, corneal ulcer or periocular infection that invades an adjacent ocular wall.3 Endogenous endophthalmitis occurs through hematogenous spread of micro-organisms that cross the blood-retinal barrier. Risk factors for endogenous endophthalmitis include the presence of systemic or local infections, relative states of immunosuppression or procedures that increase the risk of blood-borne infections.
Children account for only 0.1 percent of all cases of endogenous endophthalmitis in the United States.4 Reports of pediatric endophthalmitis are rare in the literature and are either stratified by specific etiology5-8 or single case reports. In a recent retrospective review, over a 10-year period at a tertiary referral center, only 16 cases of pediatric endophthalmitis were identified.9 No child was infected with S. aureus and all were obviously symptomatic and had clearly identifiable primary sources for their infection. The majority of cases were due to exogenous causes: either posttraumatic or postsurgical.9 Of the two cases with endogenous endophthalmitis, the children were systemically unwell. One patient was an infant with Candida sepsis, and another was immunocompromised secondary to leukemia. In children, the most commonly associated infectious sources for endogenous endophthalmitis include wound infection, meningitis, endocarditis, urinary tract infection, indwelling intravenous catheters or hemodialysis fistulas.4 To our knowledge there has only been one reported case of S. aureus in a child. This was a case of a very low birth weight neonate with sepsis.10
A diagnosis of endophthalmitis is not often suspected in otherwise healthy pediatric patients with no prior eye surgery or trauma. Combined with poor communication in pediatric patients or denial of trauma for fear of repercussion, delay in diagnosis can occur, resulting in poor visual outcomes.
In our patient, initial suspicion for infectious endophthalmitis was low, given the lack of history of trauma, hypopyon, lid swelling or significant ocular pain. The patient was otherwise healthy with no other risk factors for endophthalmitis. Additionally, our patient’s initial excellent response to both topical and intravenous steroids and then subsequent regression on an incorrectly low dose of oral steroids contributed to our thought process that he had a noninfectious, inflammatory condition. We still lack a clear source for his infection but suspect an episode of abusive eye trauma. One must always suspect physical abuse in a child when the extent of the injury is not consistent with the child’s developmental age, or the findings on physical exam do not correlate to the history.11
Infectious endophthalmitis should be considered in the differential diagnosis of pediatric patients presenting with panuveitis, even in the absence of reported trauma or other risk factors. This may be particularly important when evaluation has not otherwise determined the etiology of the uveitis. Early diagnostic vitrectomy should be considered. REVIEW
1. Kernt M, Kampik A. Endophthalmitis: Pathogenesis, clinical presentation, management, and perspectives. Clinical Ophthalmology 2010;4:121-135.
2. Yanoff M, Duker J. Ophthalmology. China: Mosby, 2009. Print.
3. Jackson TL, Eykyn SJ, Graham EM, Stanford M. Endogenous Bacterial Endophthalmitis: A 17-year prospective series and review of 267 reported cases. Surv Ophthalmol 2003;48(4):403-423.
4. Chaudhry IA, Shamsi FA, AL-Dhibi H, Khan, AO. Pediatric Endogenous Bacterial Endophthalmitis: Case report and review of the literature. J AAPOS 2006;10:491-493.
5. Alfaro DV, Roth DB, Laughlin RM, et al. Paediatric posttraumatic endophthalmitis. Br J Ophthalmol 1995;79:888-891.
6. Good WV, Hing S, Irvine AR, et al. Postoperative endophthalmitis in children following cataract surgery. J Pediatr Ophthalmol Strabismus 1990;27:283-285.
7. Recchia FM, Baumal CR, Sivalingam A, et al. Endophthalmitis after pediatric strabismus surgery. Arch Ophthalmol 2000;118:939-944.
8. Waheed US, Ritterband DC, Greenfield DS, et al. Bleb-related ocular infection in children after trabeculectomy with mitomycin C. Ophthalmology 1997;104:2117-2120.
9. Thordsen, JR, Harris L, Hubbard GB. Pediatric Endophthalmitis: A 10-year consecutive series. Retina 2008;28:S3-S7.
10. Basu S, Kumar A, Kapoor K, Bagri NK, Chandra A. Neonatal endogenous endophthalmitis: a report of six cases. Pediatrics 2013 Apr;131(4):e1292-7.
11. Waterhous W, Enzenauer RW, Parmley VC. Inflammatory Orbital Tumor as an Ocular Sign of a Battered Child. Am J Ophthalmol 1992;114:510-512.


