|
Noninfectious endophthalmitis (post-injection sterile inflammation, in which evidence of an infectious etiology was lacking and the milder clinical presentation seemed most consistent with sterile inflammation), has been reported after intravitreal bevazicumab at a rate of 0.09 percent to 1.1 percent and was reported at a rate of 0.2 percent in CATT.5-10 Noninfectious inflammation may occur more often in patients with prior history of uveitis, pseudophakia and history of vitrectomy. Several reports of noninfectious endophthalmitis after intravitreal bevacizumab injections have been documented, describing an inflammatory reaction that is often painless and recovers slowly but without permanent damage.11,12 The American Society of Retina Specialists Therapeutic Surveillance Subcommittee surveyed retina specialists’ experience during a two-month period and identified 15 eyes treated with intravitreal aflibercept that presented with sterile inflammation after the injection; however some of these eyes were treated with intravitreal antibiotics as a precaution for possible infectious endophthalmitis.13
|

Infectious endophthalmitis is defined by the presence of an infecting organism within the eye and can occur following any intraocular procedure, including intravitreal injection, surgery and trauma. Furthermore, contamination of medication batches can lead to clusters of endophthalmitis, which can have devastating visual effects. An outbreak in southern Florida occurred where 12 patients presented with symptoms of infectious endophthalmitis following intravitreal bevacizumab injection. In 10 of the 12 patients, Streptococcus was isolated from vitreous fluid.14 Each of these patients was injected with bevacizumab prepared by the same private compounding pharmacy, with all but one eye resulting in count fingers or worse visual acuity at four months of follow up.
Recently, a Georgia compounding pharmacy recalled 40 lots of its bevacizumab syringes after reports of endophthalmitis due to presumed contamination.15 This report, as well as many others, highlights the importance of adhering to the highest standards for sterile preparation of medications and injection technique, accurately identifying an infectious endophthalmitis versus a noninfectious inflammation, and treating early to avoid potential progressive vision loss from infectious endophthalmitis.16,18
Even in cases of infectious endophthalmitis, it is not always possible to identify the organism, either due to an inadequate sample of ocular fluids, poor specimen handling or difficulty in culturing the specific organism. Therefore, a “culture-negative” case of endophthalmitis may actually be infectious. In 25 to 30 percent of endophthalmitis cases, one is unable to identify an organism via culture. Infectious and noninfectious endophthalmitis can occasionally present in a similar manner in the post-injection patient, and thus, this article aims to differentiate between infectious versus noninfectious inflammation after anti-VEGF agents, based upon signs, symptoms and clinical features.
|
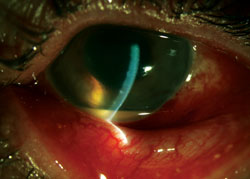
Hypopyon and Fibrin
Hypopyon has been reported as a presenting feature of infectious endophthalmitis in 78 percent of patients in one study (See Figure 1).5 Anterior chamber fibrin is uncommon in the setting of noninfectious endophthalmitis, but is very common in infectious endophthalmitis. Thus, hypopyon and/or fibrin are very strong predictors of an infectious process. With the inflammation associated with infectious endophthalmitis, there is an influx of polymorphonuclear leukocytes, aqueous flare from an influx of protein, and a conversion of intraocular fibrinogen into fibrin. Fibrin in the anterior chamber is an important finding in patients with endophthalmitis, and retraction of the fibrin (See Figure 2) after treatment is an important sign that the antibiotic therapy is effective. If an eye presents with hypopyon and fibrin, one must assume an infectious etiology until proven otherwise.
Pain
Commonly reported in these patients, pain is an early warning sign of infectious etiology. Some discomfort often occurs after intravitreal injection, but typically resolves within 24 hours. Ocular surface irritation may last longer, especially in the presence of corneal epithelial breakdown or povidone-iodine induced dryness or external inflammation after the injection procedure. Noninfectious inflammation can cause mild discomfort; however, more intense pain and deep ache after injection may suggest infectious endophthalmitis.
Vision Loss
Along with pain in the eye, another very common presenting feature is marked vision loss, shown in the Endophthalmitis Vitrectomy Study (EVS) to be present in 94 percent of postoperative endophthalmitis cases.20 Blurred vision is not as common in noninfectious endophthalmitis, but is typical in infectious cases. Vision loss can range from moderate to profound, depending on the virulence of the organism in infectious cases,21 and vision loss is less marked in noninfectious cases, if significant vitritis is present.
| ||||||
Less Common Clincal Features
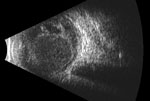
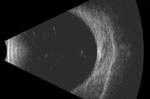
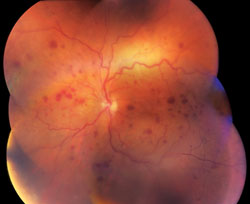
Several identifiable features are commonly seen in infectious endophthalmitis. Echography can measure the degree of vitreous opacities in these patients. Endophthalmitis in general is characterized by dense opacities, indicating the purulent infectious process. Noninfectious inflammation usually has less dense or minimal opacities. Another suggestive feature of infection is the presence of intraretinal hemorrhages, which are likely secondary to retinitis or localized venous occlusive disease. Retinal periphlebitis has been shown in clinical reports and animal models to occur early in the process of infectious endophthalmitis.22 Intraretinal hemorrhages are rarely seen as a feature in noninfectious endophthalmitis, thus their presence has positive predictive value for an infectious source. Retinal infiltrates suggest an infectious source and are commonly composed of inflammatory cells and debris from the inflammatory process.
Noninfectious endophthalmitis after intravitreal injection is a self-limited process, and resolves spontaneously after a short period of observation. This entity is well-recognized to occur after intravitreal triamcinolone injections, with an incidence as high as 0.5 percent to 2 percent of injections,23-25 and often presents with a quiet ocular surface, no fibrin and a hypopyon. This hypopyon may be true inflammatory cells or alternatively, mostly a collection of settling triamcinolone crystals, also termed a pseudohypopyon.23
In noninfectious inflammation after anti-VEGF agents, a hypopyon is typically absent and the inflammatory reaction is usually mild to moderate.19 Although a vitreous cellular reaction may be present, it usually does not obscure the view of fundus details, and it is never a dense vitritis. The B-scan echography can aid in distinguishing the level of vitritis and helping to guide the clinician to determine the nature of the vitreous opacification. Inflammation after anti-VEGF agents may be an immune reaction to the drug itself, to breakdown products in the injected material, or to an unknown contaminant.24 In cases of noninfectious endophthalmitis, the inflammatory reaction usually resolves spontaneously, typically without deleterious visual sequelae.27 Nevertheless, topical steroids may aid in a more rapid resolution of intraocular inflammation, ocular discomfort and visual loss. One report suggests that with multiple injections with anti-VEGF agents, there is a greater likelihood for generating an inflammatory response, as anti-VEGF agents are humanized antibodies.11 The four patients in that series had primarily vitreous and anterior chamber cells without fibrin or hypopyon, and the inflammation resolved with topical steroids within one to two weeks.
Since it is sometimes difficult to distinguish these two conditions, clinical judgment is the most practical source of delineation. As described in Table 1, certain pertinent features can help the clinician decide whether to use intravitreal antibiotics for infectious endophthalmitis, or reassure the patient of a benign inflammatory response. The onset of symptoms in infectious endophthalmitis typically correlates with the virulence of the causative organism. The most common infective organism following intravitreal injection is Staphylococcus epidermidis, which has been identified in one study in approximately 65 percent of endophthalmitis isolates after anti-VEGF injection.28 However, Streptococcal species have been reported as well, possibly due to needle contamination from oral flora at the time of injection.
|
The consequences of delay in treating infectious endophthalmitis can be devastating.16,17 Therefore, in borderline patients, it may be best to treat empirically with intravitreal antibiotics. In milder cases evaluated early in the course, treatment with frequent topical steroids can be considered, and the patient can be examined several hours later until the diagnosis becomes more well-defined. Ultimately, careful clinical examination and attention to subtle clinical features will guide the clinician to properly manage patients with early inflammation after injection and treat them appropriately. REVIEW
Dr. Roth is an associate professor of ophthalmology at Robert Wood Johnson Medical School, in association with New Jersey Retina. He may be reached at rothretina@gmail.com, or at the Retina Vitreous Center, 10 Plum St., New Brunswick, N.J. 08901, (732)-220-1600. Mr. Modi is a third-year medical student at Robert Wood Johnson Medical School. Dr. Flynn is a professor of ophthalmology at the Bascom Palmer Eye Institute at the University of Miami.
Dr. Roth is a consultant to Allergan, Forsight Labs, Regeneron and ThromboGenics. Dr. Flynn receives support from Santen and Vindico. This work was supported in part by the National Institutes of Health, Bethesda, Md., grant NIH P30-EY014801, and an unrestricted grant to the University of Miami from Research to Prevent Blindness, New York, N.Y.
1. Ramulu PY, Do DV, Corcoran KJ, et al. Use of retinal procedures in Medicare beneficiaries from 1997 to 2007. Arch Ophthalmol 2010;128:1335-40.
2. Moshfeghi A, Rosenfeld PJ, Flynn HW Jr, et al. Endophthalmitis after intravitreal anti-vascular endothelial growth factor antagonists: A six-year experience at a university referral center. Retina 2011;31:662-668.
3. Day S, Acquah K, Mruthyunjaya P, et al. Ocular complications after anti-vascular endothelial growth factor therapy in Medicare patients with age-related macular degeneration. Am J Ophthalmol 2011;152:266–272.
4. Chong DY, Anand R, Williams PD, et al. Characterization of sterile intraocular inflammatory responses after intravitreal bevacizumab injection. Retina 2010;30:1432-1440.
5. Fintak DR, Shah GK, Blinder KJ, et al. Incidence of endophthalmitis related to intravitreal injection of bevacizumab and ranibizumab. Retina 2008;28:1395–9.
6. Wu L, Martinez-Castellanos MA, Quiroz-Mercado H, et al. Twelve-month safety of intravitreal injections of bevacizumab (Avastin): Results of the Pan-American Collaborative Retina Study Group (PACORES). Graefe’s Arch Clin Exp Ophthalmol 2008;46:81-87.
7. Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: Two-year results. Ophthalmology 2012;119:1388-98.
8. Artunay O, Yuzbasioglu E, Rasier R, et al. Incidence and management of acute endophthalmitis after intravitreal bevacizumab (Avastin) injection. Eye 2009;23(12):2187-93.
9. Georgopoulos M, Polak K, Prager F, et al. Characteristics of severe intraocular inflammation following intravitreal injection of bevacizumab (Avastin) Br J Ophthalmol 2009;93:457-462.
10. Wickremasinghe SS, Michalova K, Gilhotra J, et al. Acute intraocular inflammation after intravitreous injections of bevacizumab for treatment of neovascular age-related macular degeneration. Ophthalmology 2008;115(11):1911.e1–1915.e1.
11. Bakri SJ, Larson, TA, Edwards AO. Intraocular inflammation following intravitreal injection of bevacizumab. Graefe’s Arch Clin Exp Ophthalmol 2008;246:779-81.
12. Kay CN, Tarantola RM, Gehrs KM, et al. Uveitis following intravitreal bevacizumab: a non-infectious cluster. Ophthalmic Surg Lasers Imaging 2011; 42:292-296.
13. Hahn P, Kim JE, Stinnett S, et al. Aflibercept-related sterile inflammation. Ophthalmology 2013;120:1100-1101.
14. Goldberg RA, Flynn HW Jr, Isom RF, et al. An Outbreak of Streptococcus Endophthalmitis After Intravitreal Injection of Bevacizumab. Am J Ophth 2012;153:204-08.
15. FDA Medwatch. Avastin Unit Dose Syringes by Clinical Specialties: Recall—Potential For Serious Eye Infection. FDA Medwatch online 2013, http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm344664.htm?source=govdelivery.
16. López-Cabezas C, Muner DS, Massa MR. Antibiotics in endophthalmitis: Microbiological and pharmacokinetic considerations. Curr Clin Pharmacol 2010;5(1):47-54.
17. Lemley CA, Han DP. Endophthalmitis: a review of current evaluation and management. Retina 2007;27:662-80.
18. Wisniewski SR, Capone A, Kelsey SF, et al. Characteristics after cataract extraction or secondary lens implantation among patients screened for the Endophthalmitis Vitrectomy Study. Ophthalmology 2000;107:1274.
19. Hoevenaars NED, Gans D, Missotten T, et al. Suspected bacterial endophthalmitis following intravitreal anti-VEGF injection: Case series and literature review. Ophthalmologica 2012;228:143-147.
20. Endophthalmitis Vitrectomy Study Group. Results of the Endophthalmitis Vitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Arch Ophthalmol 1995;113:1479-1496.
21. Johnson MW, Doft BH, Kelsey SF, et al. The Endophthalmitis Vitrectomy Study. Relationship between clinical presentation and microbiologic spectrum. Ophthalmology 1997;104:261.
22. Jeng, BH, Kaiser, PK, Lowder, CY. Retinal vasculitis and posterior pole ‘hypopyons’ as early signs of acute bacterial endophthalmitis. Am J Ophthalmol 2001;131:800-802.
23. Roth DB, Flynn HW Jr. Distinguishing between infectious and noninfectious endophthalmitis after intravitreal triamcinolone injection. Am J Ophthalmol 2008;146:346-347.
24. Roth DB, Lee SS, Flynn HW Jr. Inflammatory reactions after intravitreal triamcinolone acetonide: Possible mechanisms and therapeutic options. Expert Rev Ophthalmol 2010;5(3):273-76.
25. Nelson ML, Tennant MT, Sivalingam A, et al. Infectious and presumed noninfectious endophthalmitis after intravitreal triamcinolone acetonide injection. Retina 2003;23:686-91.
26. Johnson D, Hollands H, Hollands S, et al. Incidence and characteristics of acute intraocular inflammation after intravitreal injection of bevacizumab: A retrospective cohort study. Can J Ophthalmol 2010;45(3)239-42.
27. McCannel CA. Meta-analysis of endophthalmitis after intravitreal injection of anti-vascular endothelial growth factor agents: Causative organisms and possible prevention strategies. Retina 2011;31:654-61.
28. Sakamoto T, Ishibashi T, Ogura Y, et al. Survey of triamcinolone-related non-infectious endophthalmitis. Nihon Ganka Gakkai Zasshi 2011;115(6):523-8.
29. Ta CN. Minimizing the risk of endophthalmitis following intravitreous injections. Retina 2004;24:699-705.
30. Schimel AM, Scott IU, Flynn HW Jr. Endophthalmitis After Intravitreal Injections: Should the Use of Face Masks Be the Standard of Care? Arch Ophthalmol 2011;129:1607-1609.


