Threeplus.org
The free website Threeplus.org was created by Aaron Lee, MD, and Gokul Kumar, MD, as they completed their ophthalmology residency at Washington University in St. Louis. The site offers several options for outcomes tracking and surgical planning.
“It’s a combination of several things,” explains Dr. Kumar, currently chief resident at Washington University. “First, we wanted to create a professional networking site just for professional ophthalmologists on both an invite- and inquiry-based log-in system. You create a free account and log in with your name. Second, we wanted a free way to properly track cataract outcomes.
|
One of the first things the surgeon can do on the site is track his surgically induced astigmatism. To do this, he inputs all the variables he’d need for SIA calculation, focusing on the astigmatism amount, preexisting keratometry and the location of the incision. Next, the physician can delve into the intraocular lens calculation formulas to help choose a lens.
“If you go to the New Preop section, used for planning the next case, you first determine an identifier you want to use for the case,” explains Dr. Kumar. “Then you do the data input you’d need for the IOL calculation and determining SIA, which is basically the K readings, the axial length and the axis of astigmatism, all derived from whatever source you want. All the other data points you can enter are optional.
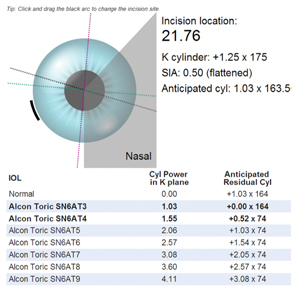
“Step three involves picking your blade,” Dr. Kumar continues. “So, people can add custom blades and see what SIAs result from their use of them. We also have default values, such as -0.5 D SIA for a 2.75-mm blade, which is what the Alcon IOL Calculator uses. Or you can have your actual data calculated, and the site will allow you to pick your blade size, incorporating your own data, or you can enter a custom blade. In the next step you pick where to put the incision. On our site, you ‘hold’ the incision virtually on the screen and move it around the cornea. As you do this, the system tells you what your anticipated residual astigmatism would be. It also tells you what your anticipated residual cylinder would be for all the current toric lenses.”
The next three steps involve lens calculations. “Pick whatever lens you want to go with, and on the back end we have all three major third-generation formulas—the Hoffer Q, Holladay I and SRK-T—and our site calculates your lenses and their anticipated residual sphere outcome,” explains Dr. Kumar. “It does this for all the data that you’ve entered, so it shows you your personalized outcome estimates as well as what the ULIB [User Group for Laser Interference Biometry] estimates would be.”
Membership on the site is by invitation, but surgeons can get an invitation by e-mailing support@threeplus.org and providing details about their ophthalmology training, contact information and current professional email address. Though the site will continuously add new lenses and other features to stay current, Dr. Kumar says it will remain easy on the wallet: “It’s a free site and we intend on keeping it free,” he says.
AAO’s IRIS Registry
Capitalizing on a trend in other medical specialties in which physicians constantly update a registry with their latest outcomes from surgery and other interventions, the American Academy of Ophthalmology is rolling out a database of its own: the Intelligent Research In Sight Registry. William Rich III, MD, the Academy’s medical director of health policy, says the system will, among other things, track outcomes with an eye toward improving them, provide opportunities for new research and help practices comply with new electronic reporting standards mandated by the government.
The key element of the registry is a program called the Systems Integrator, created by software maker FigMD. “The Systems Integrator software sits on top of the practice’s EHR program and draws out the data as it’s entered,” explains Dr. Rich. “For instance, it enters the outcomes from cataract patients and loads them into the registry without affecting the practice’s workflow.” If a practice doesn’t have an EHR program, it can enter the data via an on-line portal, though Dr. Rich acknowledges this route would be more time-consuming.
Dr. Rich says the IRIS Registry will enable practices to do some things their EHR systems do not. “The EHR doesn’t help you measure the quality of your outcomes,” he says. “For example, the registry will take every user’s input for a glaucoma patient or a cataract surgery case and, within 48 hours of completing the treatment, the physicians will be able to compare their results with anyone in their group, their region, or with a national database. That aggregated data is incredibly powerful.”
|
IRIS also allows users to slice and dice their data in different ways to look for trends. “You can see how many glaucoma patients are on generic vs. non-generics and if there’s a difference in safety or efficacy between generic and non-generic drugs,” Dr. Rich explains.
“Floppy-iris syndrome, for instance, took us almost a decade to discover,” Dr. Rich continues. “David Chang discovered he was having more complications, and had a fellow look at the records of the patients he had a complication with, and they found that these patients were 95 percent male. They then looked at their medication history and made the connection. With the IRIS Registry, you’d just have to push a button and ask: How many broken capsules are there, and is there any race, sex or use of meds in which this complication is greater? You could figure this out in a week rather than in 10 years.”
The AAO plans to roll out the IRIS Registry officially at the 2013 national meeting. The cost to be enrolled will be $500 per year. However, Dr. Rich says that, during the initial roll-out phase, the first 2,000 practices that enroll can use the registry free for two years. To find out more about the early enrollment, e-mail irisregistry@aao.org. For more information about the registry, visit aao.org/iris-registry.
Project MACULA
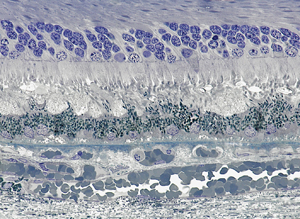
For physicians who follow patients with age-related macular degeneration, especially those who use ocular coherence tomography, it can be challenging to match up the digital images to what’s actually going on in the retina. To help make this interpretation easier, Christine Curcio, PhD, director of the AMD Histopathology Lab at the University of Alabama, Birmingham, helped create the free website Project MACULA, or MACulopathy Unveiled by Laminar Analysis.
Project MACULA is a website funded by the National Eye Institute that contains large, digitized sections of the macula taken from eye-bank specimens of wet and dry AMD, as well as from normal retinas. “It’s effectively online digital microscope views,” explains Dr. Curcio. “The idea here is to aid ophthalmologists and eye-care professionals in their interpretation of clinical imaging, such as OCT, by providing histopathology. The images are from specimens that I received from Alabama Eye Bank; they’re short post-mortem with a range of AMD pathology.” The eyes, which will eventually number 140 and come with multiple images of different layers, also have 13,000 annotations that can inform doctors about certain features of the AMD pathology and show where the features are located in relation to the OCT image. Users can zoom in on the features up close using the patented GoogleMaps technology famous for detailed geographic mapping.
Dr. Curcio says the project even revealed features never before seen: “I went through each individual section of the specimens at defined locations,” she says. “So they’ve been systematically, objectively surveyed. I crossed each layer with a vertical probe and noted what I saw. One of the big findings was subretinal drusenoid deposits. This feature had been seen clinically in patients but its histopathological correlate was uncertain before these images.”
Dr. Curcio says that the website ( http://projectmacula.cis.uab.edu/) should be done by late October 2013. “I hope clinicians find information on how to better interpret their diagnostic images from this site,” she says. REVIEW




