A 54-year-old female with chronic periocular headache presented postop day one status post frontal lobe meningioma resection with NLP vision in the left eye and a left-pupil-sparing, third-nerve palsy. The combination of NLP vision and third-nerve deficit localized the process to the posterior orbital apex and optic foramen. This localization, coupled with the mottled fundus appearance, suggested a diagnosis of a left ophthalmic artery occlusion.
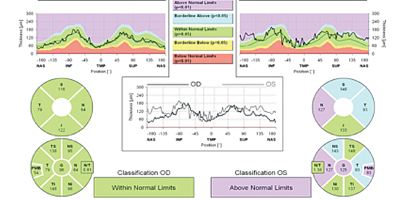
One week postoperatively, an OCT of the left optic nerve revealed moderate diffuse thickening (See Figure 1), and the fundus had a homogeneously mottled appearance (See Figure 2). The left third-nerve palsy improved in severity but the patient remained NLP with an amaurotic pupil. The patient was started on taurine and lutein supplements for potential photoreceptor regeneration.
Repeat OCT two weeks postop showed a thinned nerve head and diffusely atrophic inner and outer retinal nerve layers. The left optic nerve was pale and atrophic and the vessels were sclerotic. Three weeks postop, the patient was still NLP but the third-nerve palsy had completely resolved. The taurine and lutein supplements were discontinued.
| ||||||

Discussion
Perioperative vision loss after non-ocular surgery varies from 0.013 percent to 0.2 percent depending on the type of surgery. It occurs most commonly after cardiopulmonary bypass and spinal surgeries.1 During cardiac surgery, cholesterol plaques from re-cannulation of the aorta and microemboli from bypass circuits can infarct distal vessels. In prolonged spine surgeries, patients are often in a prone position, causing increased venous pressure and elevated intraocular pressure, which can result in subsequent ischemic optic neuropathies, cortical blindness and central retinal vein occlusions. Systemic hypotension has also been linked to vision loss. In a retrospective case-review series, patients who developed peri- or postoperative blindness had a decrease in mean blood pressure ranging from 24 percent to 46 percent for 15 minutes for up to two hours.2
In our patient, the amaurotic pupil helped localize the process to the visual system anterior to the lateral geniculate nucleus and likely to the retina or optic nerve. Disc edema on OCT suggests a diagnosis of postoperative ischemia, likely secondary to a combination of blood loss, hypotension, hypovolemia and other factors that influence perfusion to the optic disc and cranial nerve III. While operative blood loss was minimal in our patient, her blood pressure was labile, with an average systolic pressure ~100 mmHg.
Most of the blood supply to the anterior portion of the optic nerve comes from posterior ciliary arteries surrounding the optic disc. The main blood supply to the posterior optic nerve comes from the central retinal artery and pial branches, which are in turn branches of the ophthalmic artery. There is significantly less blood flow to the posterior optic nerve than to the anterior portion.3 The intracranial optic tract is supplied by branches of the Circle of Willis. Branches of the internal carotid artery and anterior cerebral artery supply the optic chiasm and optic tract, and branches of the middle and posterior cerebral arteries feed the optic radiations and occipital cortex.
A review of ophthalmic pathophysiology illustrates the importance of sustaining adequate blood pressure and hemoglobin levels. Blood flow in the choroid is the highest in the body and flows at a rate of approximately 200 mL/minute per 100 g of blood.3 Sixty to 80 percent of oxygen that supplies the retina comes from the choroid. Blood flow to the optic nerve can be measured by dividing the perfusion pressure of the globe by the resistance to flow.4 The perfusion pressure is the mean arterial pressure minus the intraocular pressure. Resistance to flow is varied by autoregulation to maintain a constant blood flow during changes in perfusion pressure. Factors that can decrease perfusion pressure and blood flow include vascular changes; increased blood viscosity; decreased oxygen delivery; overcrowding of the optic disc; and optic nerve edema secondary to nerve fiber layer hypoxia.5 Venous pressure varies with changes in body position. When the head is lower than the atrium, venous pressure increases and the perfusion pressure decreases. As a result, the choroidal blood flow simultaneously decreases.
Autoregulation operates over a critical range of perfusion pressures to limit risk of ischemic damage.4 Above or below this range, blood flow is directly dependent on perfusion pressure. Autoregulation is maintained by endothelial-derived vasoactive agents enthothelin-1, thromboxane A2, nitric oxide and prostacyclin.3 These agents are released abnormally when the endothelium is damaged. Studies have suggested that as ocular perfusion pressure decreases to less than 30 to 35 mmHg, autoregulation is disrupted and the optic nerve may become susceptible to ischemic damage.4
Types of perioperative vision loss include retinal ischemia, such as central and branch retinal artery occlusion, and ischemic optic neuropathy, such as anterior and posterior ischemic optic neuropathy. The specific mechanism and location of insult that cause ischemic optic neuropathies remains uncertain. Possible pathogenic factors include prone positioning; external pressure on the eye; long length of surgery; systemic hypotension; blood loss; hemodilution; fluid loss; and use of vasopressors.5 Uncontrolled blood loss may lead to decreased oxygen delivery to the optic nerve resulting in anterior or posterior ischemic optic neuropathy. The severity and duration of anemia that leads to this complication is unknown, but one study suggests that hemoglobin levels that dip below 8 g/dL for as little as 30 minutes may cause an optic neuropathy.3
All patients with postop vision loss need to be seen immediately. These patients should be acutely managed with transfusion of blood, supplemental oxygen and maintenance of normal-to-high systemic blood pressure. REVIEW
The author thanks Robert C. Sergott, MD, of the Wills Eye Institute’s Neuro-Ophthalmology Service for his assistance with the preparation of this case.
1. Berg KT, Harrison AR, Lee MS. Preoperative visual loss in ocular and nonocular surgery. Clin Ophthalmol 2010;4:531-46.
2. Brown RH, Schauble JF, Miller NR. Anemia and hypotension as contributors to perioperative loss of vision. Anesthesiology 1994;80(1):222-6.
3. Williams EL. Postoperative blindness. Anesthesiol Clin North America 2002;20(3):605-22.
4. Bansal AS, Hsu J, Garg SJ, Sivalingam A, et al. Optic neuropathy after vitrectomy for retinal detachment: Clinical features and analysis of risk factors. Ophthalmology 2012;119:2364-70.
5. Roth S. Preoperative visual loss: What do we know, what can we do? Br J Anaesth 2009;103 Suppl 1:i31-40. doi: 10.1093/bja/aep295.


