Diagnosis, Workup and Treatment
A workup for systemic and local herpes simplex as well as herpes zoster infection was initiated. Tests included: serum herpes simplex virus antibodies (IgM), varicella zoster virus antibodies (IgG and IgM), human immunodeficiency virus enzyme-linked immunoassay, complete blood count, conjunctival bacterial and herpes simplex viral cultures. HSV conjunctival cultures were positive, but HSV serum IgM was non-reactive. VZV serum IgG was positive and IgM non-reactive, indicating that he had been previously vaccinated and did not have an acute VZV infection. HIV was negative, CBC was within normal limits and conjunctival bacterial cultures were negative. The wound cultures sent by his dermatologist grew Staphylococcus aureus, for which he was initiated on a course of amoxicillin clavulanate.
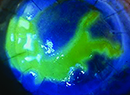
At the Wills Eye emergency room, the diagnosis of bilateral HSV keratoconjunctivitis was made. Oral acyclovir 400 mg five times daily and bacitracin zinc and polymyxin B sulfate ointment to the skin lesions twice daily were started. The following day, the Cornea Service added ganciclovir ophthalmic gel to both eyes five times daily. Within three days the corneal dendrites resolved with no epithelial defects, though he continued to feel systemically ill with subjective fevers, nausea and vomiting. After seven days of treatment, ganciclovir gel was reduced to t.i.d and continued for a total of 10 days, and acyclovir was reduced to b.i.d. Three weeks after he was seen in the emergency room only anterior stromal haze remained and corrected vision returned to 20/25 in the right eye and 20/20 in the left eye. By two months, all stromal haze had resolved and the decision was made to stop acyclovir, though consideration was given to continuing acyclovir at prophylactic dosages for the duration of his isotretinoin treatment for acne.
Discussion
Bilateral herpes simplex virus keratoconjunctivitis is an unusual manifestation of HSV infection and/or reactivation. In a 2003 retrospective observational case series of 544 patients with HSV eye disease by Paula M. Souza, MD, and colleagues, only seven patients (1.3 percent) had bilateral disease.1 They noted that all of these patients also had atopy (five out of seven), ocular rosacea (two out of seven), or another manifestation of autoimmune disease including ankylosing spondylitis (one out of seven), Crohn’s disease (one in seven), or systemic lupus erythematosis (one out of seven). However, the incidence in children and adolescents may be higher, as reported in a 2004 retrospective cohort study of 23 patients under the age of 16 years by Eva-Marie Chong, MBBS, and colleagues.2 In this study, six patients (26 percent) had bilateral HSV keratitis. Both of these studies reported significant recurrence rates, with recurrent blepharoconjunctivitis in eight eyes (57 percent) and epithelial keratitis in 12 eyes (85.7 percent) over a follow-up period of five years in the first, and 11 patients (48 percent) with at least one herpetic recurrence of either eye at a median of 15 months follow up in the second. Therefore, there is some evidence that prophylactic doses of acyclovir may be indicated in bilateral keratoconjunctivitis among both adult and pediatric populations.
Additional studies—by Fredrick T. Fraunfelder, MD, and colleagues in 2001 and more recently in 2012 by Meira Neudorfer, MD, and colleagues—have found that systemic treatment with isotretinoin may be associated with keratitis.3,4 The first study found eight cases of reactivation of herpes simplex in the setting of treatment with isotretinoin. The study concluded that although this finding could not be directly linked to treatment with isotretinoin, it certainly warrants further study. Although the mechanism for this is unclear, it may be related to altered meibomian gland secretion and impairment of tear film quality. Given high recurrence rates of HSV keratoconjunctivitis, particularly in pediatric populations, there may be a rationale for either stopping isotretinoin treatment or continuing with an antiviral medication with close ophthalmologic follow-up. It’s also important to note that ophthalmologists should be involved in the care of patients considering initiation of isotretinoin, given possible ocular side effects. REVIEW
The author would like to acknowledge Priscilla Fowler, MD, Wills Eye Cornea Service, for her time and assistance in preparing this case report.
1. Souza MF, Holland EJ, Huang AJW. Bilateral herpetic keratoconjunctivitis. Ophthalmology 2003;110:493-6.
2. Chong EM, Wilhelmus KR, Matoba AY, et al. Herpes simplex virus keratitis in children. Am J Ophthalmol 2004;138:474-5.
3. Fraunfelder FT, Fraunfelder FW, Edwards R. Ocular side effects possibly associated with isotretinoin usage. Am J Ophthalmol 2001;132:299-305.
4. Neudorfer M, Goldshtein I, Shamai-Lubovitz O, et al. Ocular adverse effects of systemic treatment with isotretinoin. Arch Dermatol 2012;148:803-8.