Intrascleral Haptic Fixation
Mesa, Arizona, ophthalmologist Yuri McKee, MD, says that Gore-Tex has a lot of potential to assist surgeons with difficult cases such as those requiring some sort of intrascleral fixation of the haptics.
 |
| Figure 1. (A) To create a Gore-Tex lasso, first punch a hole near the tail of the suture, then (B) pass the needle through the hole and (C) expose the hole to cautery to reinforce it. (D) Creating a bulb at the end of a haptic with cautery. |
“One of the problems that we run into when performing intrascleral haptic fixation,” Dr. McKee explains, “is that, with a glued IOL, sometimes there’s not enough haptic in patients with large eyes to really secure it to the sclera. The next thought is, ‘Well, just use longer haptics,’ but that would mean developing a new IOL at the cost of millions of dollars for just a limited distribution. Industry isn’t interested in doing that.” As a solution, Dr. McKee makes, in effect, a longer haptic with a Gore-Tex suturing technique. He credits New York surgeon Ken Rosenthal for being one of the first, if not the first, surgeon to use Gore-Tex in ocular surgery.
“I use a lasso technique to make a ‘longer’ haptic,” Dr. McKee explains. “The technique is useful because it doesn’t really matter what the white-to-white diameter is, because the lasso technique gives you centimeters worth of haptic, rather than just millimeters. To perform the technique, you first go to a spot near the tail of the Gore-Tex suture and poke a hole through the Gore-Tex with a 30-ga. needle. You can then take the needle itself, trailing the Gore-Tex, and pass it part of the way through the hole you’ve made, but leave the suture on the metal of the needle. Then, take low-temperature loop cautery and hold it near the suture hole where the needle passes through it—but don’t touch it. The heat melts the suture material around the needle, creating a buttonhole in the very end of the suture, which reinforces it. This is similar to the way a shirtmaker takes extra thread and sews it around the buttonhole of a shirt; the extra reinforcement around the hole prevents the hole from propagating in different directions. This step is critical, because if you were to just take the suture and poke it through its own tail and then pull on it, it tears out instantly with hardly any force being applied. But, when you make that little hole in the tail of the suture and then heat seal it, you have a very strong lasso.”
 |
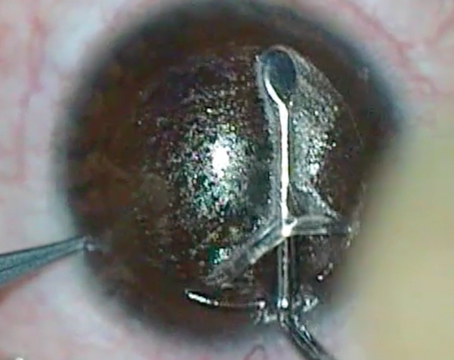
| Figure 2. (A) Looping the lasso from Fig. 1 around the haptic then pulling it tight (B). The bulb at the end of the haptic helps keep it in place. A surgical shot of an externalized haptic with Gore-Tex being run through a strut (C) and the haptic is then sutured down (D). |
To sclerally fixate an IOL, Dr. McKee first implants the IOL, then creates scleral tunnels directly opposite each other. Through one tunnel, he pulls one of the IOL haptics and snares it with the Gore-Tex suture. He then sutures down the haptic. Through the other scleral tunnel, he uses a different technique.
“With the lasso created, you have a lot of options,” Dr. McKee continues. “You can lasso an eyelet, around a haptic or through an IOL strut. I take the three-piece IOL and apply the heat loop cautery near the end of the haptic, which creates a small bulb on the end. I then take the Gore-Tex lasso and tighten it around the haptic and pull until it until it eventually stops at the little bulb I created with the cautery. This results in a surface in which there’s basically no bulk in the knot, the lasso or the connection you made between the haptic and the suture.”
 |
| Figure 3. (A, cont’d from Fig. 2) The other externalized haptic is captured with the Gore-Tex lasso and then sutured in place (B). in a second technique, multiple holes are made in the suture (C). The needle is passed through the holes and sclera, making a tight closure. |
With this in mind, Dr. McKee pulls the other haptic through the other scleral tunnel, exposes the tip to the cautery, and ties the lasso around it. “I then pass the Gore-Tex in an intrascleral pass in the same direction and plane that the haptic would have traveled in, and then double the Gore-Tex backward along that same path parallel to it,” he says. “That basically makes a haptic that would be two or three times longer than it would have been normally. Then, where it exits the sclera, I just heat-seal the tip or cut the suture, and it just flattens out to a mushroom there, making for a stable closure and extension of the haptic.”
Forget the Knot
Dr. McKee says that, when dealing with IOLs with a strut or loop such as the B+L enVista or Akreos, some surgeons pass the Gore-Tex through the strut/loop and then push it through the sclera, tie it on top of the sclera and then rotate it back into the eye. This isn’t ideal in his opinion. “For me, rotating the knot back into the eye is a problem,” he says, “because you have a full-thickness pass through the sclera, which can be a source for an infection; and you have to rotate a big knot through a small hole, which can be the source for a leak. It’s also hard to do and the suture might break.”
As an alternative, Dr. McKee makes a modification to the Gore-Tex suture that allows surgeons to get a tight closure without a knot. “I make four or five holes in a line along the tail of the Gore-Tex, separated by 0.5 mm,” he explains. “I then bring the cautery near the holes—but not touching—to strengthen them. That’s one end of the suture. I pass this through the sclera, around the loop or strut of the IOL, and then bring it back out of the sclera. Then, rather than tie it, I pass the needle through some sclera, then through one of the holes in the suture, then back through the sclera, et cetera, zigzagging it back and forth like a sewing machine, incorporating some sclera and suture with each bite. The tension created by looping your suture through four or five holes and then running it back through the sclera is actually stronger than a knot. The harder you pull it, the tighter it gets.” REVIEW
Dr. McKee has no financial interest in any of the products mentioned.