An 87-year-old Caucasian male presented to the Retina Department at Wills Eye Hospital with one month of visual distortion
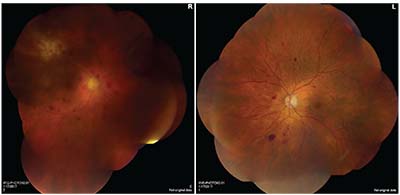 |
| Figure 1. Montage fundus photographs of the right and left eyes demonstrating severe non-proliferative diabetic retinopathy. There is an area of retinal whitening with associated hemorrhages superotemporally in the right eye. |
Medical History
Medical history was significant for poorly controlled insulin-dependent diabetes mellitus with a hemoglobin-A1C value often above 10 percent, though most recently at 7.8 percent. He also reported hypertension, coronary artery disease and valvular heart disease treated with coumadin. He was a former smoker and denied alcohol or illicit drug use.
Examination
Visual acuity was 20/60 in the right eye with no pinhole improvement and 20/30 in the left eye. The right pupil was surgically irregular and was poorly reactive, but there was no relative afferent pupillary defect. The left pupil was round and reactive. Intraocular pressure was 13 mmHg OU, motility was normal and confrontational visual fields were full OU. External and eyelid examination were normal bilaterally. On the right, corneal examination revealed small- to medium-sized keratic precipitates. The anterior chamber was deep with 3+ cell. The iris was irregular with patches of atrophy, and there was a posterior chamber intraocular lens. Anterior examination on the left was normal except for a posterior chamber intraocular lens with mild posterior capsular opacity.
Dilated fundus examination of the right eye demonstrated vitreous haze with 1+ vitreous cells. The right optic nerve appeared normal without edema or neovascularization. The macula appeared thickened, and there were scattered intra-retinal hemorrhages in the macula and throughout the periphery. There was a patch of retinal whitening in the supero-temporal mid-periphery with irregular borders and a few associated retinal hemorrhages (See Figure 1). The retinal vessels appeared mildly attenuated throughout, with a focal area of vasculitis associated with the area of retinal whitening. Dilated fundus examination on the left showed clear vitreous and a normal-appearing optic nerve. There was no macular edema, but intraretinal hemorrhages were noted to be scattered throughout the macula and periphery.
Click here for Diagnosis & Discussion.


