Our ability to help our patients often depends on technology, and one of the most useful technologies to come along in recent years is optical coherence tomography. OCT is now very commonly used by both ophthalmologists and optometrists as a means to have additional documentation of the nerve fiber layer status. Some doctors are using it to measure macular thickness and assess the status of glaucomatous damage. It can help us confirm that the visual field defect we found is not an artifact, or conversely, reveal that the structure is undamaged, so the visual field abnormality is an artifact. Sometimes OCT findings also help to reassure the patient by showing him concrete evidence that the extent of the loss is very small, or perhaps very extensive, which might make him more inclined to accept more aggressive therapy.
In the past, many doctors used instruments such as the GDx and HRT for this purpose, but today the vast majority rely on OCT instead, for several reasons. For one thing, OCT data is cross-sectional and not interpolated. The HRT uses certain floor and ceiling patterns to extrapolate the thickness of the optic nerve rim and related data; the GDx generates data by measuring polarization. In contrast, OCT gives you the actual thickness of the tissue—a real structural measure. Secondly, OCT can give you information about multiple structures, including the nerve fiber layer, optic nerve head and macula. In contrast, the GDx can only give you information about the nerve fiber layer and the HRT can only give you information about the optic nerve head.
The end result is that doctors are now making decisions about whether or not to treat—and how aggressively to treat—based on information provided by OCT instruments. But as our reliance on this technology increases, so does the cost of missing errors or overlooking shortcomings inherent in the technology. That makes it crucial for doctors to understand that OCT instruments have potential pitfalls. If we aren’t educated about these issues, we’re going to be led astray, to the detriment of our patients.
Red & Green Disease
I’m seeing the consequences of this type of error more and more frequently. People are referred to me for glaucoma diagnosis when there is absolutely no glaucoma, simply because an OCT scan was abnormal. And I’m seeing patients who have glaucoma but were told they did not have any disease because their OCT results appeared to be normal. In both situations the doctor failed to realize that artifacts were affecting what the instrument showed.
|
In fact, there are many things that can lead to erroneous results from these instruments. For starters, these are average assessments made by the computer software, and they’re based on normative databases. Normative databases are not exhaustive; they’re usually based on 300 to 500 patients. The patients in the normative database do not necessarily include high myopes, high hyperopes, children or members of different races.
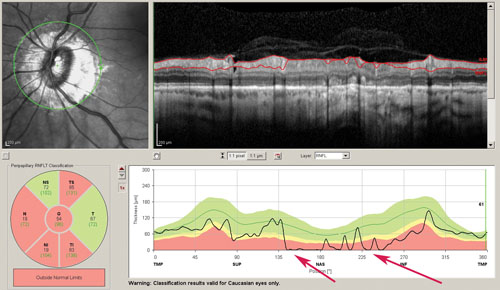
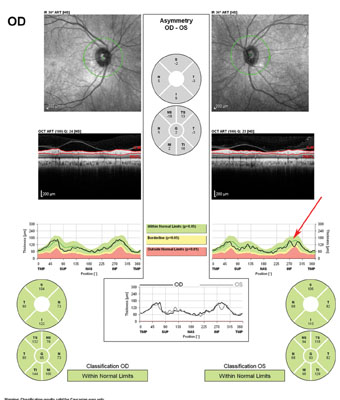
The most common OCT problem, in terms of comparison to normative databases, comes from refractive extremes, especially high myopia. High myopes’ measurements tend to fall outside of the normal range, showing up as red. On the other hand, small focal areas of damage in any eye often show up as green because the instrument averages the thickness in a particular sector. The average is often within the normal range, despite the focal loss. So the whole printout is green, giving the impression that there is no damage present.
Unless there’s a concerted effort to train people to take artifacts into consideration when interpreting the data from these instruments, we’re going to have a lot of patients being treated unnecessarily—and a lot of patients who don’t get treated when they should be.
Types of Artifacts
The artifacts that we’ve encountered most often fall into these categories:
• Acquisition-dependent artifacts. These are caused by the person who is acquiring the images. The operator, for example, may not place the ring measurement of the nerve fiber layer concentric with the optic nerve. If the ring is placed eccentrically, so that it cuts across the edge of the optic nerve, then the measurement will not read as normal. The way to avoid this problem is to have the doctor look at the raw images to make sure that the data collected is good enough to produce accurate results. The difficulty is that doctors have a limited amount of time; they can only look at so much data per patient in the clinic. However, a false report is even more time-consuming in the long run, so this really does need to be added to the doctor’s responsibilities. The doctor should look at the raw data in front of the patient, on the computer screen, as a matter of course. He can make sure it’s correctly acquired, instead of simply accepting it at face value.
• Disease-related artifacts. Sometimes the disease itself can fool the machine. The simplest example is that high myopes often have peripapillary atrophy, which may cause the software to fail to identify the nerve fiber layer in those regions.
Another common pathology-related artifact is epiretinal membranes. Although epiretinal membranes can occur in any patient, their presence is not easy to rule out because they’re just a slightly brighter layer on top of the retina. What often reveals them is the fact that they tend to be wrinkled. For that reason, if you see that the top retinal layer is wrinkled, you should assume an epiretinal membrane is present. (Of course, in some cases you may simply see what looks like a double edge to the nerve fiber layer.)
It’s also important to be sure that the software has correctly identified the upper and lower boundaries of the layer it’s scanning, because in some situations the software has trouble finding the boundaries. For example, sometimes the posterior vitreous surface that’s just above the retina will be mistakenly identified as the upper edge of the retina. You have to look at the raw data to identify where the software is placing the boundaries.
| ||||||
Managing the Problem
Despite these caveats, if you’re able to identify and compensate for the artifacts that can distort the data, OCT is a very robust technology. It can be used to not only diagnose very early glaucoma, but also to monitor progression. The artifacts can have a serious impact, but there aren’t too many of them, so it is possible to manage them. (Incidentally, very few people are using time-domain OCT—the earlier version of this technology—any more, but the same principles apply. Time domain doesn’t produce as many images, or images with as much detail, so you can be led astray even more because you’re working with less information.)
The issue is that we do have to manage this problem; we can’t just accept the data an OCT instrument gives us. We have to be willing to invest our time to look at the raw images and see how the software has analyzed it. This adds to the doctor’s burden, but powerful technology comes with responsibility. If we’re going to be able to use OCT to help us manage glaucoma, we’ll have to spend the time to make sure that what we’re getting from the machine hasn’t been altered by artifacts.
One way to manage this issue is to train technicians to check for these artifacts. We’ve done that in our office. When our technicians detect an artifact, they go to the source of the artifact and print out the extra images that are needed to identify it. They flag it “artifacts noted.” This doesn’t relieve the doctor of responsibility, but it certainly saves us time and increases the odds that false readings will be caught and corrected. (Of course, before technicians can be trained to look for these artifacts, the doctor has to recognize that this is an issue. Many doctors still are not aware that OCT artifacts are misleading them.)
As for what the future holds, these instruments are evolving as we speak. I expect that soon the instruments will identify pitfalls for us; flags will say, “Layer not identifiable” or “Note vitreous boundary.” They may not identify the pathology or the actual artifact, but they will tell us that something is wrong. I think we’ll see something along these lines soon.
Spreading the Word
OCT is a real, solid advance in glaucoma management. I can’t do my job without it. But if we want to have a major advance in technology in our armamentarium, we’re going to have to be aware of it’s shortcomings and compensate for them. To that end, education is the key. The more doctors realize that there’s a problem and learn to avoid it, the better. REVIEW
Dr. Asrani is professor of ophthalmology at the Duke Eye Center in Durham, N.C.


