Mechanisms
Subretinal hemorrhage damages tissue through a variety of mechanisms: The presence of iron, hemosiderin and fibrin in the blood has toxic effects on the overlying photoreceptors; clot retraction can sheer and damage the photoreceptors; and finally, physical separation of the photoreceptors from the RPE causes both to atrophy and can result in disciform scar formation. As the mechanisms of damage are time-dependent, early intervention is generally better.
Patients with submacular hemorrhage experience progressive visual decline. A retrospective review looked at 41 eyes with AMD-related SMH that were followed without treatment. At three years, patients lost a mean of 3.5 lines and 44 percent suffered a six-line loss of vision.3 Due to the often severe, progressive vision loss, a number of treatments have been tried. Photodynamic therapy offers the benefit of a minimally invasive, in-office procedure, but has shown uninspiring results. Patients treated with PDT for AMD-related submacular hemorrhage followed for 12 months had no significant difference between initial and final visual acuities. PDT may favorably alter the course of natural history by preventing further vision loss.4 However, visual acuity at presentation with SMH is so poor that stability alone is not an exciting endpoint.
Treatment Options
|
Dr. Heriot’s initial description of this procedure included intravitreal t-PA injection to facilitate clot liquefaction and pneumatic displacement. (Heriot WJ. Intravitreal gas and RT-PA. An out-patient procedure for submacular hemorrhage. Paper presented at: Vail Vitrectomy Meeting. 1996 Mar 10-15; Vail, Colo.) Many subsequent small case series demonstrate that the addition of 0.1 to 0.2 mL of intravitreal t-PA (either 25 μg or 50 μg/mL) can be beneficial, especially for AMD-related SMH.5-7,11 Because this technique includes the additional volume of t-PA, an aqueous tap to maintain physiologic intraocular pressure is usually required. To allow time for the t-PA to diffuse through the vitreous and lyse the clot, prone head positioning should start six hours after injection.
| ||||||

Over the past decade, anti-VEGF agents have changed the AMD treatment paradigm. Patients with thick SMH were excluded from the trials that led to Food and Drug Administration approval, however, three case series have looked at the treatment of SMH secondary to AMD with anti-VEGF alone.18-20 In each study, the investigators followed patients with AMD and SMH monthly and administered intravitreal injections of either bevacizumab or ranibizumab alone with favorable results. The authors concluded that intravitreal anti-VEGF monotherapy is superior to natural progression and is a reasonable alternative for poor surgical candidates, patients intolerant to prone head positioning or patients with subretinal hemorrhage that may be displaced directly into the fovea.
Surgical Approaches
Various surgical attempts to manage this difficult condition have been tried, including direct clot evacuation. Following pars plana vitrectomy, the clot was directly evacuated through one or more retinotomies either with or without adjuvant subretinal t-PA injection. In a few of the small case series some patients did show initial visual improvement; however, many reported significant postoperative complications, including retinal detachment, recurrent hemorrhage and subretinal fibrosis.21-24 The Submacular Surgery Trial offered a more objective evaluation as a randomized clinical trial that compared direct evacuation of the CNV/hemorrhage complex to observation and found evacuation did not stabilize or improve vision and carried a high risk of rhegmatogenous detachment.25 For these reasons this technique has largely been abandoned.
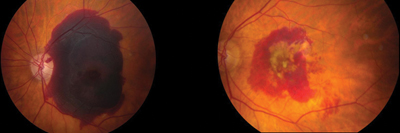
Christopher Haupert, MD, and colleagues described a hybrid surgical approach that combined the concepts of pneumatic displacement with subretinal t-PA administration in a manner that required minimal manipulation of the retina and RPE (See Figures 2 and 3).26 They described 11 cases that underwent PPV and subretinal injection of 25 to 50 μg of t-PA through a microcannula (See Figure 4) followed immediately by fluid-air or fluid-gas (SF6) exchange with postoperative prone head positioning. There was no attempt to directly evacuate the clot. The results of their series were comparable to other more invasive series and demonstrated modest visual gains in a number of patients.
Sébastien Oliver, MD, and colleagues used this approach but used only air instead of gas with shorter postoperative prone positioning. The postoperative VA results were similar to other techniques. Minimizing post-operative prone positioning improves patient satisfaction and compliance.27 Improving compliance with prone positioning in pneumatic patients is important for treatment success. Harvey Lincoff, MD, and colleagues investigated the efficacy of 40 degrees gaze down rather than face-down positioning and found it to be just as effective and considerably more tolerable.28
|
Recently, a large case series from our institution looked at 101 cases of submacular hemorrhage treated with PPV/subretinal t-PA/pneumatic gas displacement with and without post-operative anti-VEGF injections and found that 82 percent of the eyes had improvement in postoperative VA. Approximately 40 percent received anti-VEGF therapy, and these eyes showed greater VA improvement six months after surgery than those who did not receive anti-VEGF injections. The authors concluded that the addition of anti-VEGF might reduce disease progression and maintain gains made by the initial removal of submacular hemorrhage. (Garg SJ, et al. Subretinal t-PA with Pneumatic Displacement With and Without Intravitreal Anti-VEGF Agents for the Treatment of Thick Subretinal Hemorrhage Due to Exudative Age-related Macular Degeneration. The Retina Society. September 25, 2011. Rome, Italy.)
The pharmacokinetics in eyes that have had PPV differ from those that have not had PPV. Medications including anti-VEGF agents might have a shorter half-life in vitrectomized eyes, and diffusion across the SMH may be impaired. To counter this, a few case series have investigated the efficacy of subretinal anti-VEGF injections. Felix Treumer, MD, and colleagues evaluated PPV with subretinal bevacizumab and t-PA followed by pneumatic displacement and found the technique was safe and effective at displacing the hemorrhage and improving VA.29
Studies investigating adjuvant anti-VEGF therapy, either intravitreal or subretinal, suggest that postoperative treatment should include aggressive management of the underlying etiology in order to maintain the visual gains following displacement of the hemorrhage. In the case of AMD, this involves close observation and often maintenance therapy with intravitreal anti-VEGF injections.29
|

These techniques appear to be reasonably effective, but require good surgical candidates. Even with surgery, the underlying disease must be managed and the post-surgical addition of anti-VEGF medications appears to help preserve vision over time. Although the visual outcome in these patients varies widely, these strategies can help improve vision in some patients. REVIEW
Dr. Driscoll is co-chief resident of ophthalmology at Wills Eye Institute. Dr. Garg is an associate professor of ophthalmology on the Retina Service of Wills Eye Hospital and practices at MidAtlantic Retina. He can be contacted at 1 (800) 331-6634 or sgarg@midatlanticretina.com.
1. Shultz RW, Bakri SJ. Treatment for submacular hemorrhage associated with neovascular age-related macular degeneration. Semin Ophthalmol 2011;26(6):361-71.
2. Skaf AR, Mahmoud T. Surgical treatment of age-related macular degeneration. Semin Ophthalmol 2011;26(3):181-91.
3. Avery RL, Fekrat S, Hawkins BS, Bressler NM. Natural history of subfoveal subretinal hemorrhage in age-related macular degeneration. Retina 1996;16:183-9.
4. Bakri SJ, Nickel J, Yoganathan P, Beer PM. Photodynamic therapy for choroidal neovascularization associated with submacular hemorrhage in age-related macular degeneration. Ophthalmic Surg Lasers Imaging 2006;37(4):278-83.
5. Hassan AS, Johnson MW, Schneiderman TE, et al. Management of submacular hemorrhage with intravitreous tissue plasminogen activator injection and pneumatic displacement. Ophthalmology 1999;106:1900-6; discussion 6-7.
6. Hesse L, Schmidt J, Kroll P. Management of acute submacular hemorrhage using recombinant tissue plasminogen activator and gas. Graefe’s Arch Clin Exp Ophthalmol 1999;237(4):273-7.
7. Chen CY, Hooper C, Chiu D, et al. Management of submacular hemorrhage with intravitreal injection of tissue plasminogen activator and expansile gas. Retina 2007;27:321-8.
8. Ohji M, Saito Y, Hayashi A, et al. Pneumatic displacement of subretinal hemorrhage without tissue plasminogen activator. Arch Ophthalmol 1998;116:1326-32.
9. Steel DH, Sandhu SS. Submacular haemorrhages associated with neovascular age-related macular degeneration. Br J Ophthalmol 2011;95(8):1051-7.
10. Johnson MW. Pneumatic displacement of submacular hemorrhage. Curr Opin Ophthalmol 2000;11(3):201-6.
11. Ratra D, Basia A. Intravitreous tissue plasminogen activator with pneumatic displacement in submacular hemorrhage. Arch Ophthalmol 2012;130:795-6.
12. Cakir M, Cekic O, Yilmaz OF. Pneumatic displacement of acute submacular hemorrhage with and without the use of tissue plasminogen activator. Eur J Ophthalmol 2010;20(3):565-71.
13. Chen SN, Yang TC, Ho CL, et al. Retinal toxicity of intravitreal tissue plasminogen activator: case report and literature review. Ophthalmology 2003;110:704-8.
14. Gopalakrishan M, Giridhar A, Bhat S, et al. Pneumatic displacement of submacular hemorrhage: safety, efficacy, and patient selection. Retina 2007;27:329-34.
15. Kamei M, Misono K, Lewis H. A study of the ability of tissue plasminogen activator to diffuse into the subretinal space after intravitreal injection in rabbits. Am J Ophthalmol 1999;128(6):739-46.
16. Coll GE, Sparrow JR, Marinovic A, Chang S. Effect of intravitreal tissue plasminogen activator on experimental subretinal hemorrhage. Retina 1995;15:319-26.
17. Hattenbach LO, Klais C, Koch FH, Gumbel HO. Intravitreous injection of tissue plasminogen activator and gas in the treatment of submacular hemorrhage under various conditions. Ophthalmology 2001;108:1485-92.
18. Shienbaum G, Garcia Filho CA, Flynn HW Jr., et al. Management of Submacular Hemorrhage Secondary to Neovascular Age-Related Macular Degeneration With Anti-Vascular Endothelial Growth Factor Monotherapy. Am J Ophthalmol 2013;155:1009-13. doi: 10.1016/j.ajo.2013.01.012. Epub 2013 Mar 7.
19. Stifter E, Michels S, Prager F, et al. Intravitreal bevacizumab therapy for neovascular age-related macular degeneration with large submacular hemorrhage. Am J Ophthalmol 2007;144:886-92.
20. Chang MA, Do DV, Bressler SB, et al. Prospective one-year study of ranibizumab for predominantly hemorrhagic choroidal neovascular lesions in age-related macular degeneration. Retina 2010;30:1171-6.
21. Kamei M, Tano Y. Tissue plasminogen activator-assisted vitrectomy: surgical drainage of submacular hemorrhage. Dev Ophthalmol 2009;44:82-8.
22. de Juan E Jr., Machemer R. Vitreous surgery for hemorrhagic and fibrous complications of age-related macular degeneration. Am J Ophthalmol 1988;105:25-9.
23. Wade EC, Flynn HW Jr., Olsen KR, et al. Subretinal hemorrhage management by pars plana vitrectomy and internal drainage. Arch Ophthalmol 1990;108:973-8.
24. Vander JF. Tissue plasminogen activator irrigation to facilitate removal of subretinal hemorrhage during vitrectomy. Ophthalmic Surg 1992;23(5):361-3.
25. Bressler NM, Bressler SB, Childs AL, et al. Surgery for hemorrhagic choroidal neovascular lesions of age-related macular degeneration: ophthalmic findings: SST report no. 13. Ophthalmology 2004;111:1993-2006.
26. Haupert CL, McCuen BW, 2nd, Jaffe GJ, et al. Pars plana vitrectomy, subretinal injection of tissue plasminogen activator, and fluid-gas exchange for displacement of thick submacular hemorrhage in age-related macular degeneration. Am J Ophthalmol 2001;131:208-15.
27. Olivier S, Chow DR, Packo KH, et al. Subretinal recombinant tissue plasminogen activator injection and pneumatic displacement of thick submacular hemorrhage in age-related macular degeneration. Ophthalmology 2004;111:1201-8.
28. Lincoff H, Kreissig I, Stopa M, Uram D. A 40 degrees gaze down position for pneumatic displacement of submacular hemorrhage: clinical application and results. Retina 2008;28:56-9.
29. Treumer F, Roider J, Hillenkamp J. Long-term outcome of subretinal coapplication of rtPA and bevacizumab followed by repeated intravitreal anti-VEGF injections for neovascular AMD with submacular haemorrhage. Br J Ophthalmol 2012;96(5):708-13.