Background, Exam
To diagnose eyelid lesions one must first understand the anatomy of the eyelid and especially the eyelid margin and its characteristics. The eyelid margin consists of the skin, muscle, fat, tarsus, conjunctiva and adnexal structures including the approximately 100 eyelashes, glands of Zeis, glands of Moll, meibomian glands and the associated vascular and lymphatic supply.
The examination of an eyelid lesion begins with history. History should include chronicity, symptoms (tenderness, change in vision, discharge), and evolution of the lesion. Other pertinent points include a history of skin cancer, immunosuppression, fair skin or radiation therapy. Physical examination should include assessment of location, the appearance of the surface of the lesion and surrounding skin including adnexal structures. The clinician should be assessing for any ulceration with crusting or bleeding, irregular pigment, loss of normal eyelid architecture, pearly edges with central ulceration, fine telangiectasia or loss of cutaneous wrinkles. Finally, a physical examination of the patient should include palpation of the edges and/or fixation to deeper tissues, and assessment of regional lymph nodes and the function of cranial nerves II-VII. A picture can be priceless for following disease progression or response to treatment.
Although experienced clinicians may feel comfortable in their diagnosis, any doubt in clinical judgment should push the clinician for a histologic examination. Reports of clinically accurate diagnoses ranged from 83.7 percent to 96.9 percent with between 2 percent and 4.6 percent thought to be clinically benign but found to be histologically malignant.1,2
Classification
Among tumors encountered by ophthalmologist the most common neoplasms are those of the eyelid. Benign lesions of the eyelid represent upwards of 80 percent of eyelid neoplasms, while malignant tumors account for the remaining, with basal cell cancer the most frequent malignant tumor.3 It can be helpful to categorize eyelid lesions into inflammatory, infectious and neoplastic.
 |
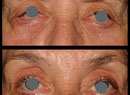
| Figure 1. Multiple chalazia located in the right lower lid of a 74-year-old female. They were treated with incision and drainage, and the biopsy was consistent with chalazion. |
• Chalazion presents as chronic, localized swelling of the eyelid and typically affects the meibomian glands or glands of Zeis (See Figure 1). Data on the frequencies is difficult to come by, but in one recent review chalazia represented nearly half of all eyelid lesions encountered in an ophthalmology practice.3 Conservative treatment with warm compresses or topical steroids is often sufficient. Surgical management includes transconjunctival incision and curettage. If excision is performed it is recommended that histopathologic confirmation of the excised lesion be performed every time.1 Alternatively, management with intralesional triamcinolone can be used although this approach carries with it complications of pigment changes or more devastating central retinal artery embolization. Intralesional dexamethasone is a safer alternative.
Infectious Lesions
• Molluscum contagiosum presents as pale, waxy and nodular cysts, classically with central umbilication. The patient is typically young, although there is increased incidence with more exuberant cases seen in AIDS patients due to reduced T cell count. They form secondary to infection from a DNA poxvirus and can present as a follicular conjunctivitis or lid nodules. The lid lesions may be misdiagnosed as a number of other eyelid lesions including basal cell carcinoma, papilloma, chalazion and sebaceous cyst. There is no predilection for the upper or lower eyelid and the local immune response will often be sufficient to eliminate the virus. Other treatment options include excision, cryotherapy or curettage.4
Neoplastic Lesions, Benign
• Squamous cell papillomas are formed from proliferation of epidermis and present either pedunculated, broad-based or white and hyperkeratotic lesions forming fingerlike projections.5 Treatment is usually not required except for cosmetic removal.
| Table 1. Malignant Eyelid Lesions Demographics and Risk Factors | |||||
| Malignant Lesions | Age | Sex Predilection | Location | Race | Risk Factors |
| Basal Cell3,12 | 70 | Equal | Lower, medial canthus | Caucasians of Celtic ancestry | Fair skin, sun exposure, smoking |
| Squamous Cell3,12 | 65 | Male | Lower | Caucasians and Asians | Fair skin, sun exposure, exposure to radiation |
| Sebaceous Gland3,14 | 65-70 | Female | Upper | Asian | Cancer syndromes and immunosuppression |
| Merkel Cell3,10 | 75 | Female | Upper | Caucasians | Immunosuppression |
| Metastasis17 | >50 | Equal | Upper slightly | None | Systemic cancer |
| Lymphoma17 | 65 | Female | No predilection | Caucasians | Systemic lymphoma |
| Melanoma18 | 60-80 | None | Lower | Caucasians | Sun exposure |
• Acquired melanocytic nevi are frequently molded to the eyelid margin and represent clumps of melanocytes at the epidermis and dermis. Not clinically apparent at birth, they increase in pigmentation at puberty. In the second decade they tend to present as elevated, pigmented papules. Later, the superficial pigmentation is lost, and an elevated, but amelanotic lesion remains.6 They usually require no treatment, but malignant transformation of a junctional or compound nevus can rarely occur and requires excision.
• Seborrheic keratosis is an acquired benign condition affecting elderly patients. Classically the lesions have a greasy and stuck-on appearance with varying degrees of pigmentation. Excision is sometimes required but recurrence is quite high.
• Hidrocystoma, also known as sweat ductal cysts, are caused by blockage of a sweat duct. They present as small (average of 4 mm) soft, smooth and transparent lesions.5,7 Eccrine hidrocystoma often present as multiple cysts along the eyelids but do not involve the eyelid margin. Apocrine hidrocystomas characteristically transilluminate, involve the eyelid margin, and are associated with a hair follicle. The apocrine variety also tend to have a bluish color with yellow deposits. Cystic basal cell carcinoma is in the differential and specimens should be sent to pathology.
• Xanthelasmas present as yellowish plaques, usually in the medial canthal areas of either the upper or lower eyelids. The plaques are filled with lipid-laden macrophages. Patients usually have normal serum cholesterol levels but it is prudent to check lipid levels, as they can be associated with hypercholesterolemia.6 Treatment options include superficial excision, CO2 laser ablation or topical 100% trichloroacetic acid.
 |
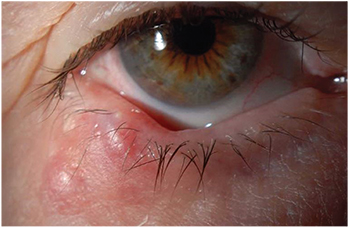
| Figure 2. Basal cell carcinoma of the left lower lid in a 57-year-old male. Note the pearly edges and central scab. Initial biopsy was consistent with BCC. The condition is treated with Mohs’ surgery with reconstruction with a Hughes flap by an oculoplastic specialist. |
• Actinic keratosis presents as round, scaly, hyper-keratotic plaques that have the texture of sandpaper. They are the most common precancerous skin lesion and usually affect elderly persons with fair complexion and excessive sun exposure. Malignant transformation for a single plaque is less than 1 percent per year.6 Observation is an option, but excisional biopsy is usually recommended to establish a diagnosis. Multiple lesions can be treated with cryotherapy, imiquimod 5% cream or other newer topical agents.
• Keratoacanthoma presents as flesh-colored papules usually on the lower eyelid in patients with chronic sun exposure or immunocompromised patients. This is now considered a low-grade squamous cell carcinoma in which dome-shaped hyperkeratotic lesions develop and can grow rapidly, with involution and regression at up to one year, once a keratin-filled crater develops.8 After diagnosis with incisional biopsy has been made, current recommendations include complete surgical excision.6
Neoplastic Lesions—Malignant
• Basal cell carcinoma represents 80 to 92.2 percent of malignant neoplasms in the periocular region.9 The localized nodular subtype is the “classic” lesion and presents most frequently on the lower lid at the medial canthus as a firm, raised, pearly nodules with fine telangiectasias (See Figure 2).11 A less common form of BCC, but more locally aggressive is the morpheaform type; these lesions lack ulceration, and appear as an indurated white to yellow plaque with indistinct margins.8
Patients are typically middle-aged or older and often fair-skinned, although it can occur in children and persons of African ancestry.12 BCC in younger patients has a more aggressive growth pattern and does not demonstrate the latency period seen in older patients.12 Treatment is primarily with Mohs’ micrographic surgery followed by eyelid/facial repair with oculoplastics.
Orbital invasion occurs in less than 5 percent of BCC and most commonly the lesions are at the medial canthus.8,12 Signs of orbital invasion include a fixed orbital mass, restrictive strabismus and globe displacement or destruction.9 CT or MRI is indicated to determine the extent of the disease. Once penetration reaches deep to the septum, local excision is very difficult. Nests of basal cells often hide, and this leads to more aggressive surgery (including orbital exenteration). Some cancer centers prefer external beam radiation followed by surgical removal in these advanced cases.
• Squamous cell carcinoma is the second most common eyelid malignancy, occurring in the lower lid approximately 60 percent of the time.13 SCC lacks the pathognomonic features, which allows for differentiation from precursor lesions including actinic keratosis, Bowen’s disease (squamous cell cancer in situ) and radiation dermatitis.8,12 The presentation is often with a painless nodular lesion with irregular rolled edges, pearly borders, telangiectasias and central ulceration, similar to BCC.12 The clinical diagnosis has been reported to be accurate anywhere from 51 percent to 62.7 percent of the time.13 Patients are generally males older than 60 and often have a history of other skin lesions requiring excision.11
Predisposing factors include both extrinsic factors, such as ultraviolet light, exposure to arsenic/hydrocarbons/radiation, HPV infection or immunosuppressive drugs and burns; and intrinsic factors of albinism and xeroderma pigmentosa.11,13 Metastasis of the lesions is most commonly through the lymphatic system, and early detection of lymph node involvement is essential to improve the prognosis.9,11 SCC invades along the trigeminal, oculomotor and facial nerves and can present as asymptomatic perineural invasion detected on histologic examination or symptomatic perineural invasion. SCC with perineural invasion has a recurrence rate of up to 50 percent, and postoperative radiotherapy for all SCC with perineural invasion has been suggested.9
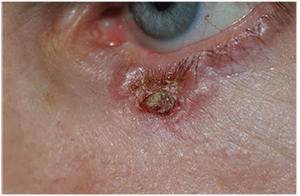
• Sebaceous carcinoma originates in the meibomian glands or the glands of Zeis and presents clinically as yellowish discoloration due to its lipid content; it can mimic blepharoconjunctivitis, chronic chalazia, BCC, SCC or other tumors (See Figure 3).8 The lesions most commonly affect women aged 65 to 70 in along the upper lid.14 It can present as loss of eyelashes, destruction of Meibomian orifices or chronic unilateral blepharoconjunctivitis. SC affects all races, but Asians in particular, and represents the most common or second most common periocular malignancy in this group.3,9
The diagnosis can be missed on initial biopsy, and may require multiple biopsies or special stains. Superficial biopsy is often not sufficient and can miss the underlying tumor; therefore a pentagonal full-thickness excision or punch biopsy may be necessary to make the diagnosis. Biopsy specimens with intraepithelial involvement of the conjunctiva should raise the suspicion for orbital invasion.8
 |
| Figure 3. Sebaceous carcinoma of the left lower lid in a 52-year-old female. Patient presented with chronic unilateral blepharoconjunctivitis for 12 months, madarosis and eyelid lesion. Incisional biopsy showed sebaceous gland carcinoma. Definitive treatment should be undertaken by an experienced oculoplastic specialist or multidisciplinary team. |
• Merkel cell carcinoma of the eyelid presents in elderly Caucasian women, average age of 75, with immunosuppression being a risk factor. Half of all MCCs are located in the head and neck, and between 5 and 10 percent occur in the eyelids.10 MCC presents in the upper lid as a painless, red-purple vascularized nodule, sparing of the overlying epidermis. In 20 to 60 percent of patients, there is lymph-node positivity at presentation and distant metastases appear within two years 70 percent of the time.15 This can be an aggressive, fatal cancer that requires judicious biopsy and systemic management by oncology.
Tumor size and metastasis at presentation are the most important prognostic factor with MCC tumors. The evaluation for tumor-lymph node-metastasis starts after the histologic diagnosis. Regarding treatment, the tumor responds well to radiation therapy, but primary treatment of the tumor is with excision and wide margins or Mohs’ surgery.10
• Metastasis to the eyelid is rare and represents less than 1 percent of malignant eyelid tumors; it usually occurs in the course of widespread metastatic disease, but can be the presenting sign of systemic cancer. The features of metastasis to the eyelid are not specific and can be solitary or multiple eyelid nodules or diffuse eyelid swelling. Biopsy should always be considered. Breast and cutaneous melanoma are the most common primary carcinomas.16
• Lymphomas of the ocular adnexa are primary tumors involving the orbit. Lymphoma presenting on the eyelid is rare and usually associated with systemic disease. Lymphoma of the eyelid represents 10 percent of ocular adnexal lymphoma.17
• Melanoma of the eyelid is a relatively rare tumor, making up less than 1 percent of eyelid cancers.5 Lesions present in a patient in the sixth to eighth decade of life as a pigmented and thickened area of pigment on the lower eyelid with irregular borders.10,18 In any patient with a pigmented lesion, biopsy should be considered. REVIEW
Dr. Notz is a staff associate in ophthalmology at Geisinger Health System. Contact him at 100 North Academy Ave. Department of Ophthalmology, Danville, PA 17822. E-mail: gmnotz@geisinger.edu. Dr. Kasenchak is a second-year ophthalmology resident at Geisinger. E-mail: jekasenchak@geisinger.edu.
1. Kersten RC, Ewing-Chow D, Kulwin DR, Gallon M. Accuracy of clinical diagnosis of cutaneous eyelid lesions. Ophthalmology 1997;104:479-84.
2. Margo CE. Eyelid tumors: Accuracy of clinical diagnosis. Am J Ophthalmol 1999;128:635-6.
3. Deprez M, Uffer S. Clinicopathological features of eyelid skin tumors. A retrospective study of 5504 cases and review of literature. Am J Dermatopathol 2009;31(3):256-62.
4. Charteris DG, Bonshek RE, Tullo AB. Ophthalmic molluscum contagiosum: Clinical and immunopathological features. Br J Ophthalmol 1995;79:476-81.
5. Eagle R. The eyelid and lacrimal drainage system. In: Eye Pathology: An Atlas and Text. Philadelphia: LWW, 2011:241-242.
6. Shields JA, Shields CL. Eyelid, Conjunctival, and Orbital Tumors. An Atlas and Textbook. LWW; Third edition October 9, 2015
7. Singh AD, McCloskey L, Parsons MA, Slater DN. Eccrine hidrocystoma of the eyelid. Eye (Lond) 2005;19:77-9.
8. Bernardini FP. Management of malignant and benign eyelid lesions. Curr Opin Ophthalmol 2006;17(5):480-4.
9. Slutsky JB, Jones EC. Periocular cutaneous malignancies: A review of the literature. Dermatol Surg 2012;38:552-69.
10. Missotten GS, de Wolff-Rouendaal D, de Keizer RJ. Merkel cell carcinoma of the eyelid review of the literature and report of patients with Merkel cell carcinoma showing spontaneous regression. Ophthalmology 2008;115:195-201.
11. Harvey DT, Taylor RS, Itani KM, Loewinger RJ. Mohs micrographic surgery of the eyelid: An overview of anatomy, pathophysiology, and reconstruction options. Dermatol Surg 2013;39:673-97.
12. Cook BE Jr, Bartley GB. Treatment options and future prospects for the management of eyelid malignancies: An evidence-based update. Ophthalmology 2001;108:2088-98.
13. Donaldson MJ, Sullivan TJ, Whitehead KJ, Williamson RM. Squamous cell carcinoma of the eyelids. Br J Ophthalmol 2002;86:1161-5.
14. Snow SN, Larson PO, Lucarelli MJ, Lemke BN, Madjar DD. Sebaceous carcinoma of the eyelids treated by Mohs micrographic surgery: Report of nine cases with review of the literature. Dermatol Surg 2002;28:623-31.
15. Missotten GS, de Wolff-Rouendaal D, de Keizer RJ. Merkel cell carcinoma of the eyelid review of the literature and report of patients with Merkel cell carcinoma showing spontaneous regression. Ophthalmology 2008;115:195-201.
16. Bianciotto C, Demirci H, Shields CL, Eagle RC Jr, Shields JA. Metastatic tumors to the eyelid: Report of 20 cases and review of the literature. Arch Ophthalmol 2009;127:999-1005.
17. Stefanovic A, Lossos IS. Extranodal marginal zone lymphoma of the ocular adnexa. Blood 2009;114(16):3499-3500.
18. Vaziri M, Buffam FV, Martinka M, Oryschak A, Dhaliwal H, White VA. Clinicopathologic features and behavior of cutaneous eyelid melanoma. Ophthalmology 2002;109:901-8.