In the past, when a patient presented with lower-lid issues that required blepharoplasty, our approach was similar to just buying clothes off the rack—very limited and, often, one-size-fits-all. Now, however, our treatment paradigm is much more like having a suit custom-tailored to our exact taste and dimensions. Specifically, there’s been a transformative shift from a primary focus on subtraction to the value of the addition of volume in periorbital aesthetics.1-4 An appreciation of midfacial volume loss, gravitational descent and skin textural changes all should inform the surgeon’s approach, which can then be individualized to a specific patient’s facial changes.5,6
Here, I’ll explain the various ways you can customize patients’ lower-lid blepharoplasty surgery, based on their individual ocular and facial needs.
Evaluating the Patient
Addressing any anatomic patient concern should first begin with defining the underlying causes, and lower-eyelid aesthetics is no exception.
Not all eyelids are created equal. In fact, patients may require anything from superficial laser resurfacing or a chemical peel to address just skin textural changes, to hyaluronic acid filler or fat transfer for volume restoration, to surgical intervention with liposculpting and transposition with or without skin resection—or any combination of the above.
The examination should focus on understanding the particular aging changes that have resulted in the configuration that’s troubling to the patient. The history should focus on understanding the patient’s specific concerns about their lower eyelids. After all, what bothers the surgeon may not bother the patient, and vice versa. Therefore, establishing this relationship and understanding is essential to planning a successful cosmetic surgery.
 |
Preoperative evaluation of the lower eyelids requires identifying how each feature of facial aging determines the bothersome changes to the lower eyelid-midface complex. Defining how the identified clinical findings relate to the overlying and underlying anatomic changes will guide the treatment plan. Beginning with the skin and working posteriorly to the changes of the underlying bony anatomy will permit a consistent, systematic approach.6
Aging changes to the periorbital skin may be accentuated relative to the rest of the face due to the lack of substantial dermis in this location, along with its intimate relationship to the underlying orbicularis and associated ligaments. Skin aging becomes manifest due to a loss of hyaluronic acid, loss of collagen and loss of elastin. All of these changes contribute to reduced elasticity, and the increased laxity and wrinkling observed over time.7 Additional features, particularly in photodamaged skin, include irregular pigmentary changes, as well as dullness and roughness.7 Depending on the severity of the skin changes, intervention may involve skin resection or adjuncts to surgery, including a chemical peel or laser resurfacing.
Beneath the skin, the ligamentous structures of the lower eyelid undergo important and involutional changes.6 These changes can result in lower eyelid laxity and increase the propensity for postoperative ectropion or retraction if the laxity goes unrecognized preoperatively and isn’t addressed at the time of surgery.6 Therefore, the degree of lower eyelid laxity should be assessed preoperatively and dealt with at the time of surgery, if necessary. To maintain optimal postoperative lower eyelid position, consider performing surgical maneuvers focused on preserving orbicularis integrity for paralysis prevention and incorporating lateral canthal tightening, if necessary.6 The presence of concomitant floppy eyelid syndrome may necessitate more extensive intraoperative tightening procedures such as the formation of a true lateral tarsal strip.
Managing Orbital Fat
Among the biggest shifts in recent years has been the change in the surgeon’s approach to the prominent appearance of the orbital fat pads. It was previously thought that with aging comes fat herniation and prolapse. Instead, this change in contour along the eyelid-midface junction relates more to the surrounding prominences and hollows.1-6 A combination of liposculpting and transposition of the orbital fat can be a more thoughtful and conservative approach that will prevent postoperative hollowing over the long term.1-6,8,9
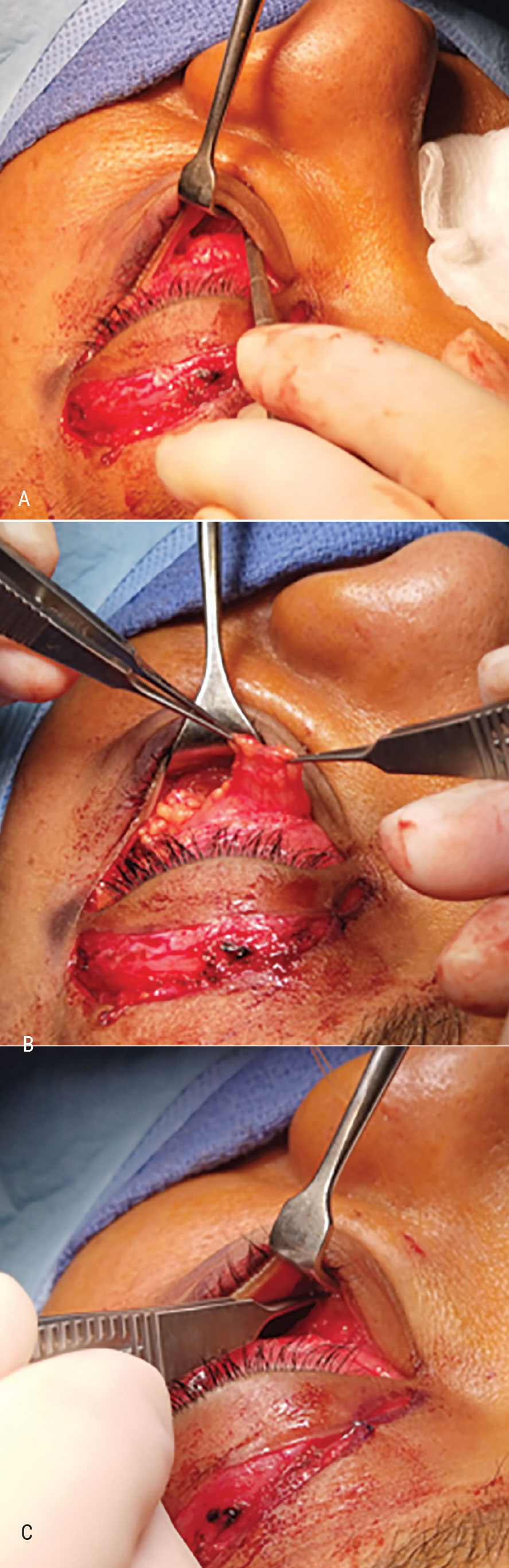 |
| Figure 1. Intraoperative views of a transposition lower blepharoplasty with ligament release and sub-periosteal pocket development (A), fat pedicle development (B), and the pedicle transposed into the subperiosteal space (C). Ligamentous release and pocket development can also be performed in a pre-perisoteal plane. Depending on the degree of surrounding volume loss, supplementing surgery with additional volume restoration through autologous fat transfer or adjunctive hyaluronic acid filler may be necessary to optimize the contours in the region. Click image to enlarge. |
Figure 1 (right) demonstrates intraoperative views of a transposition lower blepharoplasty with ligament release and sub-periosteal pocket development (A), fat pedicle development (B) and the pedicle transposed into the subperiosteal space (C). Ligamentous release and pocket development can also be performed in a pre-periosteal plane. Depending on the degree of surrounding volume loss, you may need to supplement surgery with additional volume restoration through autologous fat transfer or adjunctive hyaluronic acid filler in order to optimize the contours in the region.8,9 A dynamic preoperative assessment of the appearance of the lower-eyelid fat in up- and down-gaze can help determine the amount of fat present, as well as aid in distinguishing fat from edema. In up-gaze, the fat will prolapse forward and become more prominent than in down-gaze. This is in contrast to chronic edema, which will remain constant with globe position. This examination is similarly useful for identifying areas of necessary fat preservation, subtraction and transposition. Gently balloting the globe can further help to reveal compartments with excess fatty tissue.
Festoons
Differentiating between fat and edema is essential to managing appropriate patient expectations, and certainly informs the planned surgical approach. Lower eyelid edema, particularly in the malar region, has garnered much attention due to the challenges it presents in terms of definitive management. Festoons are postulated to form as a result of changes to the surrounding ligamentous structures in the prezygomatic space.10 Specifically, edema is thought to collect in a well-demarcated triangle in the malar region due to the relative laxity of the superior orbital retaining ligament with the maintained strength of the inferior zygomatico-cutaneous ligament.10 Malar festoons are a common source of patient concern and may be the focus of their lower eyelid cosmetic goals.
The options for festoon management range from the most invasive and definitive—direct excision—to less-invasive approaches focused on the principles of sclerotherapy.
Direct festoon excision, as the name implies, involves incising around the margins of the festoon and excising it directly. This technique can be performed in isolation or as an adjunct to lower blepharoplasty. This approach has proven to be effective for festoon management,11,12 but is limited by patient tolerance for an aggressive approach that involves waiting for their visible incision line to fade along the relaxed skin tension lines.
An alternative surgical approach that’s also proven effective involves employment of a subperiosteal midface lift in conjunction with an orbicularis muscle-skin flap.13,14
Non-surgical interventions include radiofrequency approaches, thermoplasty, laser resurfacing and trichloroacetic acid chemical peels.13
More recently, injection of sclerosing agents has shown promise in the management of malar festoons.15,16 The use of intra-lesional tetracycline (2%) resulted in improvement in 21 patients, as determined by photo evaluation by blinded graders.15 This treatment was noted to be well-tolerated, without any complications.15
A similar study was conducted for the investigation of the efficacy and safety of intralesional doxycycline; it demonstrated a statistically significant improvement in festoons, without complications.16 Compared to tetracycline, doxycycline has the benefit of enhanced accessibility, and it can be reconstituted in the office.16 The precise mechanism of action behind the tetracycline family of antibiotics with regard to their utility as sclerosing agents isn’t fully elucidated, but they’ve been shown to induce collagen and fibrin deposition, leading to fibrosis.16
Unfortunately, regardless of the treatment approach, one of the most important things to manage when it comes to festoons is the patient’s expectations, because these pockets of edema can be elusive and notoriously refractory to treatment.
Dealing with Ligaments and Volume Issues
Lastly, the structural bony changes and areas of volume loss will help guide the degree of necessary fascia ligament release and volume augmentation by fat autologous grafting or postoperative hyaluronic acid filler. In one report, University of Texas Southwestern Medical Center’s Joel Pessa, MD, and his colleagues identified specific changes to the skeletal facial structure that occur with aging and how these changes affect alterations observed in the overlying soft tissue and ligamentous structures.17 Over time, they noted that the lower maxillary skeleton at the piriform becomes retrusive relative to the upper face,17 and the maxillary wall from the orbital rim to the inferior zygoma tilts further posteriorly.17 Lastly, the medial orbit becomes more anteriorly positioned.17
It’s postulated that the aforementioned changes in the bony skeleton result in changes in the overlying muscles, ligaments and soft tissues, as bony changes may alter the location of tendinous insertions. For example, the malar mound and nasojugal fold (also known as the “tear trough”) are thought to be accentuated as a consequence of the positional shift in the plane of the maxillary wall.17 Tendon repositioning may also cause a change in the position of the malar and buccal fat pads.17 All of these soft tissue structures are also undergoing their own simultaneous involutional changes.
Restoring the effacement of the lower eyelid and cheek by addressing these volume changes is important for optimizing lower blepharoplasty.18 Midfacial projection ideals are defined by the golden ratio of facial aesthetics. Tel Aviv, Israel’s Ran Stein, MD, co-authored a study that demonstrated the value of autologous fat grafting to the inferior orbital rim, the deep and medial fat pads, and Ristow’s space as a means to optimize facial proportions in this region.18
The nasojugal and malar folds are defined by the cutaneous attachments of the orbicularis retaining ligament (ORL). The nasojugal fold begins at the inner canthus and is formed by the depression between the orbicularis oculi muscle and levator labii superioris muscle.19 The malar fold begins at the outer canthus toward the inferior aspect of the nasojugal fold.19 With age, ligaments lose strength and elasticity, resulting in the descent of the surrounding soft tissues. This causes elongation of the vertical height of the lower eyelid and prominence of the nasojugal and malar folds.19
 |
The orbicularis retaining ligament is responsible for the overall shape of the lower eyelid. Changes in the ORL are variable along its course and, since it’s typically weakest centrally, result in more prominent bulging of the inferior orbital fat pads in this region.19 The degree of ligamentous laxity also varies among the different facial ligaments. Although the zygomatic cutaneous ligaments undergo some attenuation with age, they remain strong relative to the ORL. Therefore, descent of tissues from ORL weakness will meet the stronger zygomatic ligament, resulting in malar mound formation.19
Release of the ORL during lower-eyelid blepharoplasty makes conceptual sense from the standpoint of eliminating a physical boundary separating the lower lid from the cheek and dividing what was once a single, continuous, youthful unit.
Several authors have demonstrated the effectiveness of ORL release as an adjunct to lower-lid blepharoplasty in order to address the tear trough.6,20 One of the limitations of several of the articles on this technique is the lack of comparison to patients who underwent lower blepharoplasty without ORL release. In one study, however, researchers compared the efficacy and complications in patients with and without ORL release. They concluded that ligamentous release didn’t enhance the aesthetic outcome and could pose an increased risk of prolonged swelling and chemosis as well as increase the risk of lid malposition.20
Ultimately, successful lower-eyelid/midface rejuvenation is dependent upon a solid understanding of the patient’s goals, clearly defining and managing the patient’s expectations of what can be achieved, and taking a thoughtful, systematic, and anatomy-based approach to rejuvenating the region. The advances in our understanding of the changes that occur in the face with aging have permitted a three-dimensional approach to rejuvenation, in order to optimize patient outcomes
beyond what was achieved with subtractive approaches alone. Fitting the surgery to the patient’s expectations and specific anatomic aging changes permits a customized surgery that addresses their aesthetic goals and functional needs, allowing them to achieve the best possible outcome.
Acknowledgement: I’d like to acknowledge the profound influence of my great mentor Tanuj Nakra, MD, FACS, whose biplanar systematic approach to lower-eyelid blepharoplasty has defined the framework of my approach to lower-lid rejuvenation, and has helped me develop the methodical guide described in the article.
Dr. Watson welcomes questions and comments on the article. Please direct correspondence to:
Wills Eye Hospital, 840 Walnut Street, Suite 910, Philadelphia, PA 19107
Phone: 215-928-3171
Fax: 215-928-3454
Email: awatson@willseye.org
1. Loeb R. Fat pad sliding and fat grafting for leveling lid depressions. Clin Plast Surg 1981;8:757.
2. Hamra ST. Arcus marginalis release and orbital fat preservation in midface rejuvenation. Plast Reconstr Surg 1995;96:354-362.
3. Kossler AL, Peng GL, Yoo DB, Azizzadeh B, Massry GG. Current trends in upper and lower eyelid blepharoplasty among American Society of Ophthalmic Plastic and Reconstructive Surgery members. Ophthal Plast Reconstr Surg 2018;34:37-42.
4. Hartstein ME, Massry GG. The lift and fill lower blepharoplasty. Ophthal Plast Reconstr Surg 2012;28:213-218.
5. Goldberg RA, McCann JD, Fiaschetti D, et al. What causes eyelid bags? Analysis of 114 consecutive patients. Plast Reconstr Surg 2005;115:1395–402 (discussion: 1403–4).
6. Nakra T. Biplanar contour-oriented approach to lower eyelid and midface rejuvenation. JAMA Facial Plast Surg 2015;17:5:374-381.
7. Ganceviciene R, Liakou AI, Theodoridis A, Makrantonaki E, Zouboulis CC. Skin anti-aging strategies. Dermato-endocrinology 2012;4:3:308-319.
8. Cicui PM, Obagi S. Rejuvenation of the periorbital complex with autologous fat transfer: Current therapy. J Oral Maxillofac Surg 2008;66:8:1686-1693.
9. McCracken MS, Khan JA, Wulc AE, et al. Hyaluronic acid gel (Restylane) filler for facial rhytids: Lessons learned from American Society of Ophthalmic Plastic and Reconstructive Surgery member treatment of 286 patients. Ophthal Plast Reconstr Surg 2006;22:3:188-191.
10. Medelson BC, Muzaffar AR, Adams WP Jr. Surgical anatomy of the midcheek and malar mounds. Plast Reconstr Surg 2002;110:885-896 (discussion: 897-911).
11. Einan-Lifshitz A, Hartstein ME. Treatment of festoons by direct excision. Orbit 2012;31:5:303-6.
12. Bellinvia P, Klinger F, Bellinivia G. Lower blepharoplasty with direct excision of skin excess: A five-year experience. Aesthetic Surg J 2010;30:665-670.
13. Krakauer M, Phil M, Aakalu VK, Putterman AM. Treatment of malar festoon using modified subperiosteal midface lift. Ophthal Plast Reconstr Surg 2012;28:459-462.
14. Hoenig JF, Knutti D, de la Fuente A. Vertical subperiosteal mid-face-lift for treatment of malar festoons. Aesthetic Plast Surg 2011;35:522-529.
15. Perry JD, Mehta VJ, Costin BR. Intralesional tetracycline injection for treatment of lower eyelid festoons: A preliminary report. Ophthal Plast Reconstr Surg 2015;31:50-52.
16. Godfrey KJ, Kally P, Dunbar KE, et al. Doxycycline injection for sclerotherapy of lower eyelid festoons and malar edema: Preliminary results. Ophthal Plast Reconstr Surg 2019;35:474-477.
17. Pesa JE, Zadoo VP, Mutimer KL, et al. Relative maxillary retrusion as a natural consequence of aging: Combining skeletal and soft-tissue changes into an integral model of midfacial aging. Plast Reconstr Surg 1998;102:1:205-212.
18. Stein R, Holds JB, Wulc AE, et al. Phi, fat, and the mathematics of a beautiful midface. Ophthal Plast Reconstr Surg 2018;34:491-496.
19. Jordan DR, Mawn L, Anderson RL. Surgical Anatomy of the Ocular Adnexa: A Clinical Approach. 2nd edition. Oxford University Press, 2012:55-69.
20. Chan NJ, Nazemzadeh M, Hartstein ME, et al. Orbicularis retaining ligament release in lower blepharoplasty: Assessing efficacy and complications. Ophthal Plast Reconstr Surg 2018;34:155-161.


