Dr. Miyake spoke about his work with two breakthrough technologies that allow multiple surgeons and students access to high-definition, 3-D viewing of ocular surgery—while using far less light inside the eye, minimizing any chance of retinal phototoxicity. The first new technology is a high-gain avalanche rushing-amorphous photoconductor (HARP) camera capable of capturing high levels of detail with far less light than standard cameras. The second is a single-camera, high-definition 3-D television system. The two technologies, created at the Japan Broadcasting Co. and the NHK Science and Technical Laboratories in Nagoya and Tokyo, have now been successfully used together during multiple surgeries on human patients.
We asked Dr. Miyake to explain how the two technologies work, and to provide an update on their use and development.
High-definition, Low Light
According to Dr. Miyake, the HARP camera is 600 times more sensitive than older, standard cameras. A standard camera pickup tube—the device that registers the incoming light—is about 4 µm deep and uses an electric field of 1.25 x 107 volts per meter. A photon entering the tube triggers the release of one electron hole pair, whose impact on the far side of the tube is registered by the scanning beam.
In contrast, the HARP camera's tube is 25 µm deep and uses a more powerful electric field of 108 V/m, which accelerates each electron hole pair generated by the arrival of a photon. The acceleration causes impact ionization, which generates additional electron hole pairs as it travels across the tube, until 600 pairs have been generated by the impact of a single photon. Thus, far less incoming light can produce a bright, clear image.
In previously published studies,1 experimental surgeries were performed using a prototype of this system under different light intensities. The surgeon and two observers evaluated whether the different levels of light allowed adequate visualization for safe and effective surgery. They found that cataract/
intraocular lens surgery could be performed using 7.3 percent (about one-fourteenth) of the illumination required with a standard camera, and vitrectomies could be safely performed using less than a third of the light necessary with a standard camera. The latter may be especially significant, since long-term studies have found that retinal phototoxicity is most severe after vitreoretinal surgery.2 (In fact, the HARP camera is so sensitive that levels of illumination normally used with a standard camera interfered with clear visualization.)
 |
| A new stereo optical system sends left and right images through a single camera; the images are then seen by the surgeon (and any other observers) using stereo viewers that require no special glasses. Kensaku Miyake, MD |
Also, the HARP camera provides a wider view of the surgical field than previous cameras.
Seeing Through a Stereo Viewer
The second new technology captures the stereo images from a microscope and transmits them through a single high-definition TV camera using an optical adapter that combines the left and right eye images with a prism, image rotator and lens. (In contrast, conventional 3-D systems use two sets of cameras, recorders and projectors.) An optical adapter at the viewing end presents the information stereoscopically in a viewing port, designed so that each eye sees only the appropriate image. As a result, no special glasses are needed; the viewer only has to look into the HDTV stereoscopic viewer.
The surgeon watches his work through one of these viewers as well, rather than looking directly through the microscope. Thus, the low-light enhancement provided by the HARP camera works to everyone's advantage, including the surgeon's, and all viewers see exactly what the surgeon is seeing.
"The HD 3-D single-camera system has multiple advantages," notes Dr. Miyake. "First, team surgery is possible, since multiple individuals can all see exactly what the surgeon is seeing. Second, the images can be viewed by remote surgeons, in real time, to obtain expert recommendations during the procedure. Third, video can be compiled for future educational use. Finally, additional relevant information can be superimposed onto the visuals to assist the surgeon, such as phaco or vitrectomy machine settings."
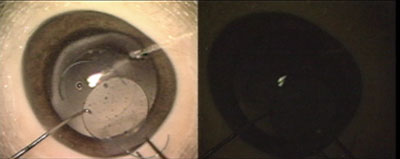 |
| The HARP camera (left image) is 600 times more sensitive than a standard camera (right image). These images were captured with 1/100 the illumination normally used during cataract surgery. Kensaku Miyake, MD |
In Practice
Although some of the technology has been available since 1999, Dr. Miyake says his team did not try using the pair of new technologies during surgery on humans until two years ago. So far, he says they've done about 10 cases. "We have now used this system during actual human operations including both cataract/IOL surgeries and macular surgeries," he explains. "We've found it very effective, particularly in terms of the low illumination.
"We've also tried using the instrument as a tool for training and educating young surgeons, and when performing team surgery," he says. "These technologies have been very useful in both situations. Students report that they are learning more than they did before we incorporated these viewing capabilities."
For the surgeon, looking into a stereoscopic viewer during surgery is a significant change from looking into a microscope. "Some find it more comfortable than the microscope," says Dr. Miyake. "It doesn't take any time to get used to it, and some users report less eyestrain and backstrain."
Dr. Miyake notes that the system is still being improved; they are working to reduce the size and weight of the HARP camera and improve the resolution of the stereoscopic viewer. "This technology could also be used with a slit lamp," he adds, "but we haven't tried that yet." He expects it will be several more years before the current system with the HARP camera and stereo viewers reach the marketplace.
Upcoming Developments
Dr. Miyake and his team have also been using a new ultrahigh-speed, high-sensitivity camera under development by researchers in Japan, Germany and the Netherlands. This camera lets them photograph processes that occur too quickly for the eye to follow, such as ablation of corneal tissue during refractive surgery. Previous versions of the new camera had increased its sensitivity beyond earlier high-speed cameras by a factor of 10; the latest prototype has increased the sensitivity yet again by another factor of four. The result has a pixel count of 300,000 with a maximum speed of 1 million frames per second.
This technology was originally designed to provide slow-motion playback of televised sporting events even under low lighting at night; it has the added advantage of providing sufficient density of data to meet the specifications of high-definition television broadcasts. But like many technologies, its most important use may turn out to be as a powerful tool for scientific research.
1. Miyake K, Ota I, et al. Application of a Newly Developed, Highly Sensitive Camera and a 3-Dimensional High-Definition Television System in Experimental Ophthalmic Surgeries. Arch Ophthalmol 1999:117;1623-1629.
2. Postel EA, Pulido JS, Byrnes GA, et al. Long-term follow-up of iatrogenic phototoxicity. Arch Ophthalmol 1998:116;753-757.


