It doesn’t happen as much anymore. When LASIK went mainstream in the 1990s, post-LASIK epithelial ingrowth rates were much higher in patients. The complication is characterized by the ingrowth of corneal epithelium at the interface between the flap and the stromal bed. Current prevalence rates range from 0 to 3.9 percent after primary LASIK, but can range from 10 to 20 percent after retreatment.1 Here, refractive surgeons discuss today’s approaches for epithelial ingrowth removal, and what considerations, if any, should be given to retreatment with LASIK in light of the higher ingrowth rates.
Do Nothing
“Epithelial ingrowth is very rare after primary LASIK,” explains Andrew I. Caster, MD, FACS, medical director, Caster Eye Center Medical Group in Beverly Hills. “Yet, it’s very common to have a little bit of peripheral epithelial ingrowth on a secondary flap-lift case. Frequently it only extends a millimeter from the edge, maybe two millimeters. In these cases, it really has no clinical impact.
“Therefore, if the epithelial ingrowth is peripheral and the refraction is very good, then I won’t treat the epithelial ingrowth,” Dr. Caster continues, adding that he’ll schedule the patient for follow-up in a month or two. “I’ll tell them to come back earlier if there are any problems, but most of the time it’s asymptomatic and doesn’t require treatment.”
When Is It Cause for Concern?
“Epithelial ingrowth can be evident as soon as one week after a LASIK procedure but sometimes it doesn’t appear for a month or more,” explains Dr. Caster. “And sometimes there can be late-onset epithelial ingrowth, appearing six months to 12 months after a procedure, but that’s rare.”
So, when is ingrowth an issue? “Occasionally epithelial ingrowth will extend further in, and then it can have an effect on the refraction; lifts up the flap in that area and can cause astigmatism. That’s what I would call clinically relevant epithelial ingrowth,” warns Dr. Caster. “I find in my retreatment cases that it’s around 10 percent overall. It’s even more common when you’re doing a hyperopic retreatment.”
Epithelial ingrowth risk increases in retreatment candidates who had a mechanical keratectomy, which is associated with “a smaller optical zone and a smaller-sized flap,” says Dr. Caster, adding that “the angle of the flap at the edge isn’t very large. It’s less perpendicular to the plane of the cornea, a common scenario with older keratomes.”
LASIK done with a femtosecond laser has made a difference. “Flap surgery with a laser seems less likely to cause epithelial ingrowth because [flaps] have a more definitive edge to them and that may serve as a barrier to the incursion of epithelium at the interface of the flap,” notes John Hovanesian, MD, in practice at Harvard Eye Associates in Laguna Hills, California. To help avoid ingrowth problems, procedure choice is also a factor. “The choice of what refractive procedure to use depends on surgeon preference, experience and the level of suspicion that the patient will have regrowth,” he adds.
Another risk factor for epithelial ingrowth is eyelid conditions. “Conditions such as meibomian gland dysfunction, blepharitis, any external inflammation and dry eyes—all of those increase your risk of epithelial ingrowth after a LASIK flap lift retreatment,” notes Dr. Caster.
Approaches to Ingrowth Removal
“The hardest part of the procedure is identifying the edge of the flap. Sometimes it can be hard to find,” explains Dr. Caster, adding that indirect lighting can help. “If you bounce the light off of the iris or the limbus you get lighting throughout the cornea. That will illuminate the flap edge, which is hard to see with direct illumination.” Another approach is to use the elbow of a Sinskey hook to put pressure on the cornea. “You’ll see an indentation where the flap edge is.” In rare cases, Dr. Caster says you can go into the OR and use the Sinskey hook to scrape away some of the epithelium “and the Sinskey hook will grab onto the edge of the flap,” but he cautions that this method can cause corneal abrasion.
Dr. Caster first identifies the edge of the flap. Then, once under the operating microscope, “I take a Sinskey hook and move it around all 270 degrees of the flap,” he says. “You try not to drag epithelial cells underneath the flap, so as you move the Sinskey hook around, you pull up on it. Then I go in with a spatula and free up the entire flap, lifting it up and getting it out of the way.”
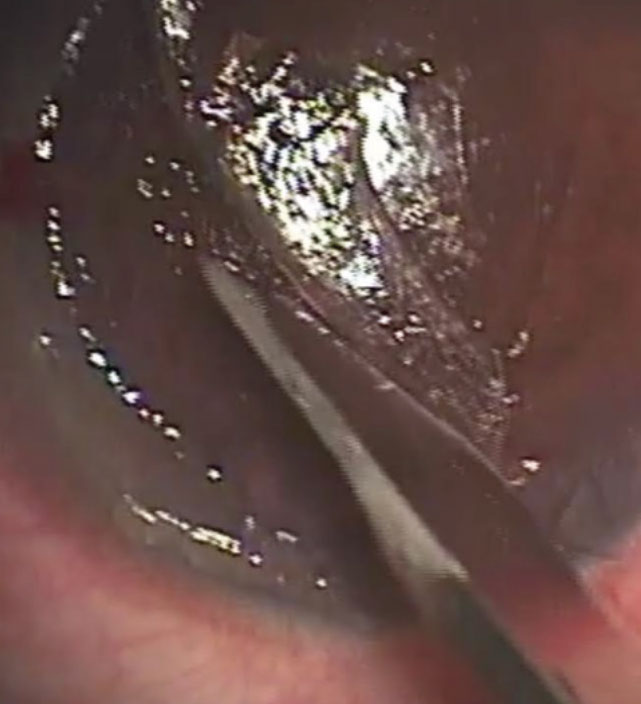 |
| Figure 1. Dr. Hovanesian uses a no.15 blade to scrape epithelium from underneath the flap interface. |
However, Dr. Hovanesian says it’s not always necessary to lift the entire flap. “Sometimes you can just lift it in the area of the ingrowth,” he notes. “To remove the ingrowth, we typically scrape with a blunt spatula, although you can use a sharp blade, but at an obtuse angle so that you don’t damage tissue.” Essentially, he says, “The effort is to scrape away epithelium, both from the bed and from the backside of the flap, where we may have remnants of epithelium (See Figure 1). We try to remove epithelium from the site where it grows from underneath the edge of the flap. We’ll often debride a little of the epithelium on the [corneal] surface as well, just to move it away from the edge of the flap and lessen the chance that it will find its way back down.”
“A lot of times the epithelium is very soft, and you can just use some dry Weck-Cel (BVI) sponges to wipe it away. Otherwise you can use a hockey-stick-shaped instrument to free up the epithelial cells,” says Dr. Caster. He wipes it all off and then goes back with a dry sponge to get any epithelium hanging over the edge. If there’s a lot of epithelium, he’ll go to the underside of the flap and scrape it with a sponge or a hockey-stick instrument.
“In recalcitrant cases I will remove the ingrowth and then glue and suture the flap down,” says Dr. Hovanesian. (See Figure 2) “The idea is to close the conduit. The glue fills that space for a few days and maybe retards the advancement of the epithelium. The idea is that two stromal surfaces will close a little more completely, preventing epithelium from reentering the previously opened door.”
Dr. Caster says he doesn’t remove a thin rim around the edge of the epithelium. “We want to seal this thing back down without the epithelium growing underneath,” he explains. “You want to accomplish your goal with the minimum amount of manipulation to avoid swelling.” He doesn’t use sutures or glue. “I’ve not had to resort to suturing the end of flaps or other more aggressive treatments,” he remarks. “This simple way of removing epithelial ingrowth has worked in my hands.”
 |
| Figure 2. In this same procedure, Dr. Hovanesian has already sutured down the flap, and is applying the thrombin component of fibrin tissue adhesive to the ocular surface. The full procedure can be viewed at https://youtu.be/fW-iuWZCQeM. |
Others have investigated approaches that don’t require lifting the flap. Dr. Hovanesian recalls the work of Jorge L. Alio, MD, from Alicante, Spain, who’s published on his experience with the YAG laser method, which uses low-energy laser bursts targeted toward the flap interface to induce scarring to shrink the space between the flap and the bed.3
Risk and Retreatment Considerations
Refractive surgeons who are risk-averse to epithelial ingrowth may alter their retreatment plans. “A lot of surgeons follow the one-year rule,” notes Dr. Hovanesian. “If it’s after one year, they don’t lift a flap because of concerns about epithelial ingrowth.”
Dr. Caster describes his approach: “If I’m doing a hyperopic retreatment, I explain to patients that the risk of epithelial ingrowth could be higher than 10 percent,” he says. “And I present the alternative, which is to do a PRK.” Although he typically prefers LASIK, Dr. Caster says, “If I were going to do a large hyperopic retreatment where the initial flap was done with an older mechanical keratome, I might lean towards the PRK.”
Ideally, it comes down to eliminating the need for retreatments. “We lived through some challenging times in the early days of LASIK,” recalls Dr Hovanesian. “But we’ve been refining techniques, laser platforms have improved, and now we’re seeing very high rates of accuracy. We don’t do as many enhancements, so because enhancements have gone down, epithelial ingrowth has gone down.”
1. Santaella R, Feldman BH, Santaella RM, et al. Post LASIK epithelial ingrowth management. AAO EyeWiki. Jan 20, 2015. https://eyewiki.aao.org/Post_LASIK_Epithelial_Ingrowth_Management Accessed October 12, 2021.
2. Ting DSJ, Srinivasan S, Danjoux JP. Epithelial ingrowth following laser in situ keratomileusis (LASIK): Prevalence, risk factors, management and visual outcomes. BMJ Open Ophthalmol 2018;3:e000133. Published March 29, 2018
3. Ayala MJ, Alio JL, Mulet ME, et al. Treatment of laser in situ keratomileusis interface epithelial ingrowth with neodymium:yttrium-aluminum-garnet laser. Am J Ophthalmol 2008;145:4:630-634.


