Presentation
An asymptomatic 8-year-old Asian Indian male was seen for a routine examination by the local ophthalmologist. On fundus evaluation, the physician noted a choroidal pigmentary abnormality in both eyes and referred the patient for evaluation at the Ocular Oncology Service at Wills Eye Hospital to rule out malignancy.
Medical History
 |
This patient was the product of a full-term pregnancy with uncomplicated prenatal, perinatal and postnatal courses. Past medical and surgical histories were unremarkable. Iris heterochromia was noted at 1 month of age with a blue iris in the right eye and brown iris in the left. When the patient was 6 years old, his primary ophthalmologist noticed choroidal pigmentary abnormalities in both eyes and recommended observation. Family history was remarkable for diabetes mellitus and hypertension on the maternal side. He had no known allergies or medications. There was no family history of vitiligo, albinism, Waardenburg syndrome or other pigmentary abnormalities. There was no family history of cancer.
Examination
 |
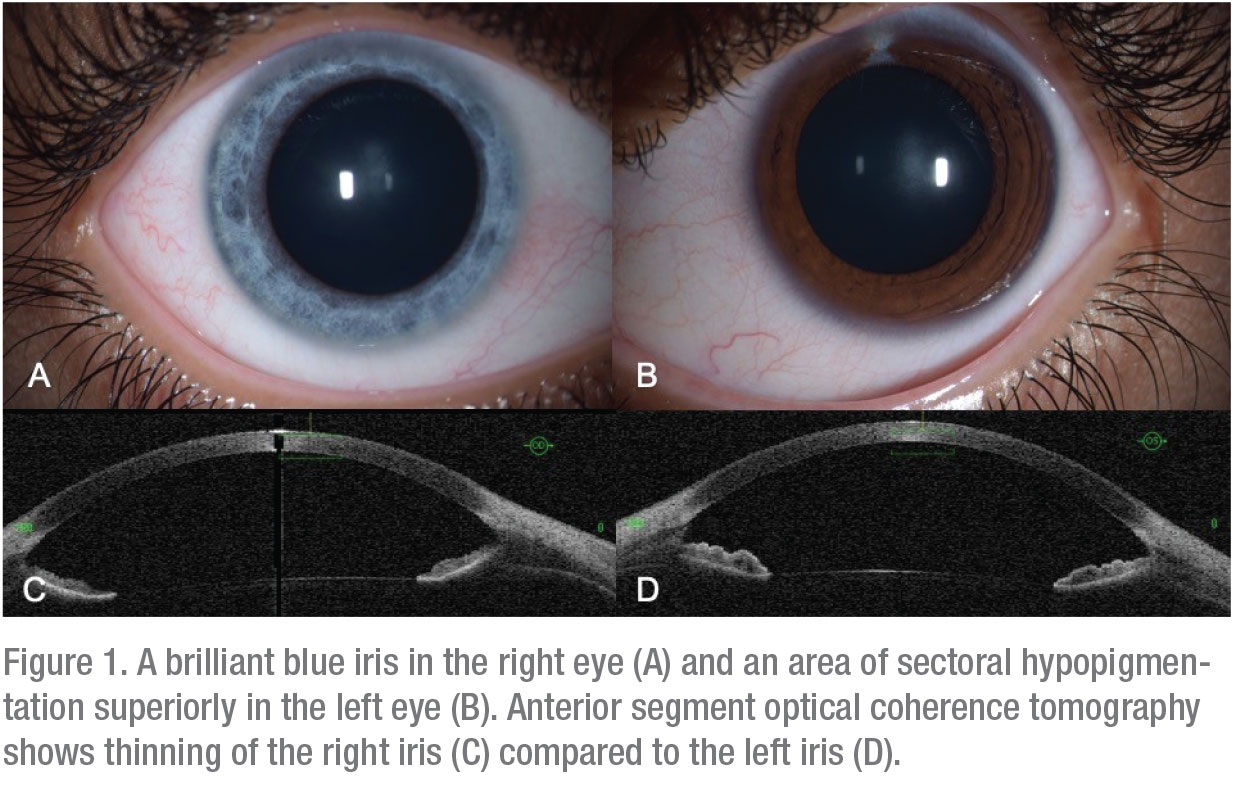
On ocular examination, visual acuity was 20/20 OU. Both pupils were round, equal and reactive. Intraocular pressure was normal to finger tension OU. Confrontation visual fields and ocular motility were full bilaterally. The anterior segment examination of the right eye revealed a “brilliant-blue” iris, despite his Asian Indian heritage (Figure 1A). The left iris was homogeneously brown with a focal segment of pigment loss superiorly, appearing blue (Figure 1B). The rest of the anterior segment examination was unremarkable.
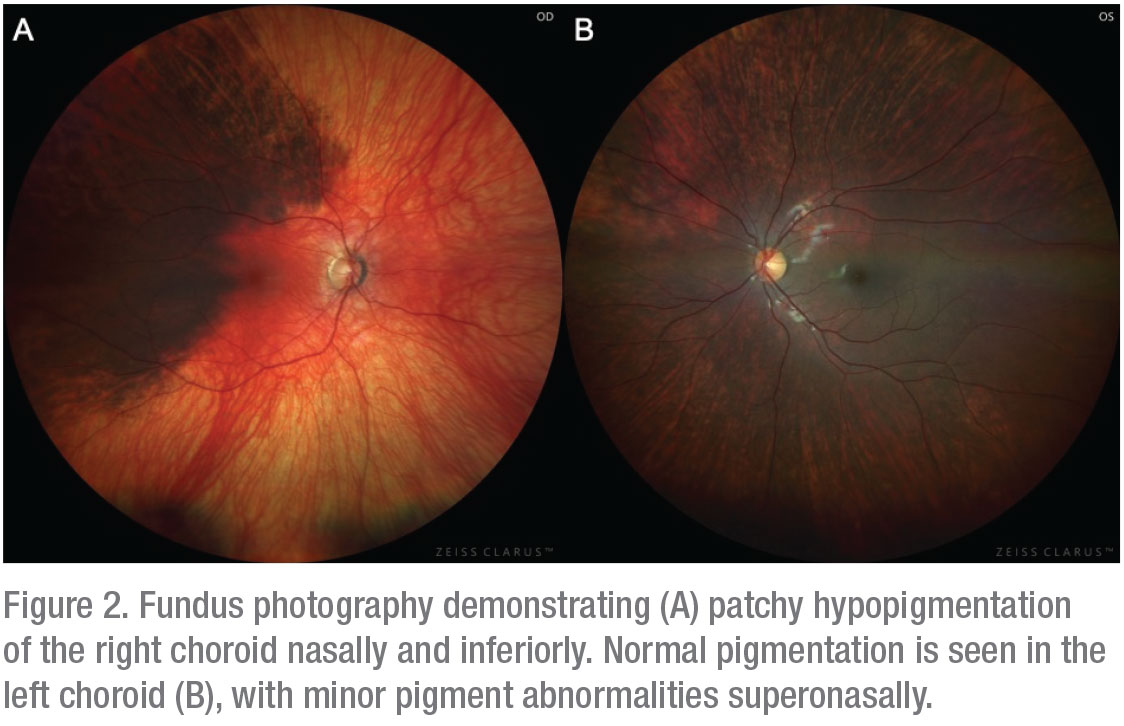
On funduscopic examination, patchy diffuse choroidal hypopigmentation was noted with preserved normal pigmentation superotemporally in the right eye (Figure 2A). There was no subretinal fluid, orange lipofuscin pigment, choroidal mass, retinal pigment epithelial abnormalities or peripheral drusen. The left fundus had normal pigmentation with subtle, wedge-shaped hypopigmentation superonasally (Figure 2B).
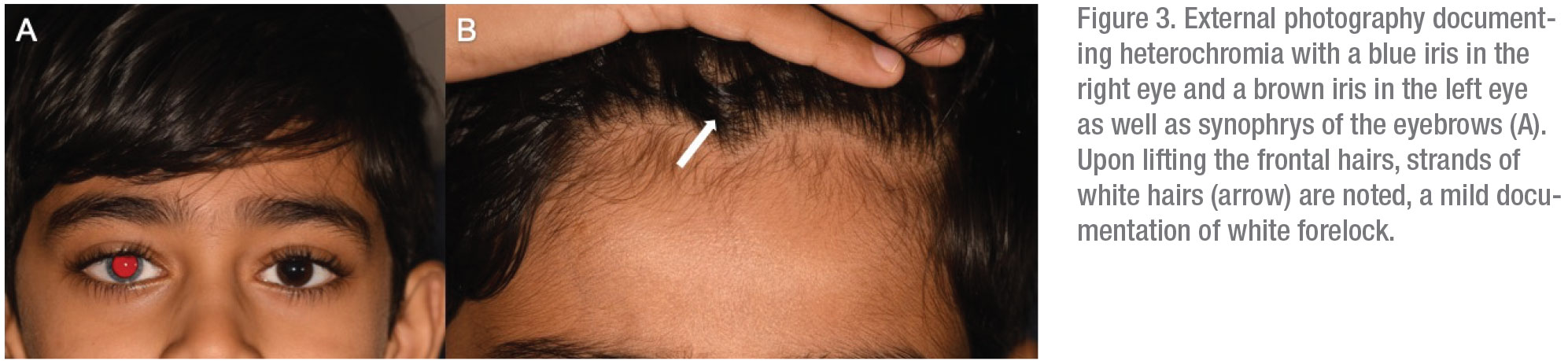
An external examination found mild synophrys with eyebrow hairs over the upper nasal bridge (Figure 3A). Upon careful examination of his scalp hair, there was trace evidence of a white forelock (Figure 3B, arrow). Otherwise there was no displacement of the medial canthi, no broad nasal root or any other dermal or palatal hyper- or hypopigmentation. There was no skeletal deformation, and a hearing test was normal.
 |
What is your diagnosis? What further workup would you pursue? Please click this link for diagnosis, workup, treatment and discussion.


