There is no question that capsular tension rings are of great benefit in complicated cataract cases. These devices, approved for use in the United States in October 2003, are a significant leap forward in handing cases of weak zonules, allowing surgeons to place an intraocular lens safely in the capsular bag. While recognizing that the CTR has given us a new confidence in managing complicated cataract cases, they may have also given us a false sense of security. In certain cases, if the CTR is used improperly, we will run into intraoperative issues and long-term postop complications. It's clear that CTRs have not necessarily made cataract surgeries foolproof. In this article, I'll draw on my five years of CTR experience in Canada to recount what I consider to be the top four complications of working with the rings, and review my preferred way to deal with each of them.
#1. Capsular Bag Tear
As with all surgical procedures, success results from a combination of good technique and careful patient selection. Iatrogenic creation of a tear by the insertion of the CTR is a problem of technique. Complications resulting from poor patient selection include complete dislocation of the lens into the vitreous cavity, or postop IOL dislocation due to significant weakness pre-surgery or progression of zonulysis.
Remember that the CTR puts the capsule on stretch, increasing centrifugal forces. Thus, the posterior capsule may be relatively anterior to what you're used to, increasing the risk of an inadvertent capsular tear. Be aware of this during phacoemulsification and cortical aspiration.
 |
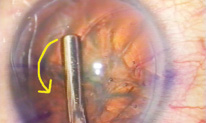
| Cortical aspiration in the presence of an implanted CTR may require tangential stripping, with contraction of the CTR to strip equitorial cortex. Often, cortex may need to be accessed posteriorly. |
• Working space. With enough pressure and torque, even the gently curved CTR can go through a thin capsule. In my opinion, problems are more common when the CTR is implanted prior to lens removal, known as "early" insertion. With insertion early in the case, with the cataractous lens still present, it follows that you need to create room to work, making adequate hydrodissection and viscodissection key. The importance of working space increases with a very dense cataract. If you have no room in the bag and you're trying to implant the CTR, you are more likely to go through the bag or you may damage existing zonules.
Typically the BSS used in cortical-cleaving hydrodissection isn't sufficient to create enough space in the bag to implant a CTR. I recommend using a viscoelastic, particularly a cohesive viscoelastic like Healon GV (Pfizer Ophthalmology) to move and spread tissue. This will create room in the capsular bag and provide enough lubrication to implant the CTR.
• Dialing technique. Most CTR implantation methods involve a dialing technique. If you feel any resistance as you move it along the capsular equator, it's likely that the ring is going to catch at the equator and go through the bag if enough force is put behind it. The bottom line is to stop if you feel any resistance. Go back and do more viscodissection, or consider implanting the ring "late" in the case, utilizing capsular hooks or a capsular tension segment instead. I'll discuss these techniques later.
• Existing tears. Do not implant a capsular tension ring in the presence of an existing anterior or posterior capsule tear. While the tear may be located anteriorly, it's still of concern, because if you put enough tension on the capsule while dialing in the CTR, you're going to cause that tear to extend posteriorly—rupturing the capsular bag and resulting in complete loss of capsular support. Posterior capsular tears may extend further, and thus a CTR should not be implanted in such cases unless you perform a posterior capsulorhexis.
• Capsulorhexis size. Because the capsulorhexis is the aperture through which we implant the CTR, a very small one can lead to trouble. If the capsulorhexis is very small, during insertion you're putting extra tension on the capsulorhexis edge, risking a tear in the capsule. It's also important to perform a large-sized capsulorhexis in these loose-zonule cases to reduce the severity of postop capsular contraction. My recommendation is to create a capsulorhexis around 5.5 mm.
 |
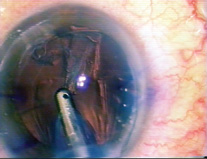
| To prevent excessive capsular bag torque and possible equatorial tear or further dialysis, a "backing out" approach is preferred for CTR injection. |
#2. Retained Cortex
Quite often, it can be difficult to cleave cortex from the capsule during hydrodissection when using a CTR. After the ring is implanted, the ring can trap the cortex. Usually the irrigation/aspiration tip is enough to do it, but a CTR acts as a buttress against cortical removal. Because the CTR is designed to expand in the capsular bag, it presses the cortex into the equator, making removal difficult and trying the surgeon's patience. A couple of things can help in this situation.
• Separation prior to implantation. You can prevent entrapment of the cortex by using adequate viscodissection. With viscoelastic, try to separate the cortex from the capsule prior to implantation of the ring. If you can implant the ring behind the cortex, removal of cortex will be easy because it's been pulled away and now sits in front of the ring. This is not easy to do and results are not always consistent. It also can take a lot longer than typical cortical removal in the routine case.
• Other stripping techniques. Attempt tangential cortical stripping. Rather than pulling toward the center of the capsule, pull along its equator. Slide it back and forth, trying to move the cortex sideways along the ring. Often that is just enough to loosen it. Another choice is to remove it along the posterior capsule. While we typically remove cortex anteriorly, often you need to go posteriorly and remove cortex. If necessary, one may need to pull the CTR centrally to free up cortex.
#3. Iatrogenic Zonular Damage
Patient choice and technique are equally important in avoiding this particular complication. When you have a dense, thick cataract, you have very little room in the capsular bag in which to work with the CTR. Any forces placed within the bag are easily transmitted to the zonules because there is no space in which those forces can be absorbed. This is of concern because the zonules are already damaged. Any additional force or tension could cause further loss and might be enough to actually cause the capsular bag to dislocate, or at least become partially dehisced.
• Timing of implantation. While this is an area of some controversy, I believe in avoiding "early" implantation of the CTR in a very dense lens. With weak zonules and a dense cataract, remove the cataract first and then implant the ring. I have shown in my Miyaki-Apple video analysis of CTR insertion that, in these cases, you can create more damage to the zonules by implanting a CTR early in the case.
• Hooks and retractors. To support the zonules during phaco, some surgeons use multiple iris hooks at the capsulorhexis edge to act as synthetic zonules. Since a very small area of the hook holds the capsulorhexis edge, many surgeons will use the force of several hooks. There is still risk of capsular tears and dislodgment from the force applied with the hooks, so the surgeon using this method should be on his guard.
• Capsular tension segment. In general, I find that hooks and retractors often cause more problems than they solve. That's why I designed the capsular tension segment, a 90-degree PMMA partial ring segment that has a 4.5- or 5-mm radius of curvature (See sidebar). The CTS eliminates the problems with tears and dislodgment related to use of hooks for support.
#4. Inadequate Capsular Centration
Unfortunately, it's too easy to transform someone with only three clock hours of zonular weakness into someone with six clock hours if you create further zonular damage. This may happen by implanting the ring "early" in a dense lens case, or by torquing the bag as you implant the CTR.
• Suturing the implant. You may succeed with a CTR (or a CTS) at reforming the capsular bag, but if the zonules themselves are so weak that they can't support the bag, it will be out of position. Centration does require at least some zonular support to provide the tension to hold the bag in the proper place. As a general rule, you should suture the implant in a case where there is more than 90 degrees or three clock hours of zonular dialysis, or where the zonular weakness may be grossly evident.
| Capsular Tension Segment | |
| Dr. Ahmed's capsular tension segment is a further modification to the capsular tension ring developed by Robert J. Cionni, MD, for cases in which a CTR wouldn't be appropriate. After capsulorhexis and before phacoemulsification, the surgeon may implant up to three (in severe cases) capsular tension segments to support the capsule over weakened zonules. An iris retractor, placed through the fixation eyelet on the CTS, can further increase stability during lens removal. Once used, the CTS may be removed, or may be sutured over an area of zonular weakness for continuing support. While the CTS is not currently approved for use in the United States, investigation continues. Visit morcher.com for details. |  |
Another concern is that a CTR may not prevent progressive zonulysis conditions and late postoperative IOL decentration. You can use either a modified Cionni ring or a capsular tension segment, either is ideally suited for these cases. However, since neither of these devices is available in the United States as of this writing, the best you can do is wisely select patients according to zonular risk, and modify your technique in ways that I recommend below.
• Manual vs. injector insertion. There are two ways to implant the capsular tension ring, each with implications for capsular tears and excessive torque on the capsular bag: manual or with an injector. I have shown via Miyaki video that the injector method is much less traumatic than manual insertion.
Injecting the CTR will be rather straightforward for those surgeons familiar with IOL injection systems. You place the CTR injector into the eye, slowly depressing the plunger, pushing the ring forward through the capsular bag, thereby dialing it around the capsular equator.
• Back-away approach. To mediate the force used in this injection (avoiding further damage to the zonules and puncture with the ring as in complication #1) I recommend a back-away approach. Place the tip of the CTR forward until you meet some resistance then back away in a circular fashion, moving the injector around rather than keeping it fixed and moving the ring forward. As you pull backward and press the plunger, you are using the body of the ring to put it into position.
• Direction of insertion. When you're injecting the ring, it's helpful to inject it "towards" the area of greatest weakness. If you inject away from the area of greatest dialysis, you are more likely to create further tension and possible additional zonular damage.
Moving Forward
Early on in the use of capsular tension rings, I believe we thought that CTRs might do more than they actually can. We assumed that once you put the CTR in, you could reposition the dislocated capsular bag. We assumed we could prevent capsular phimosis and fibrosis. We presumed CTRs were benign to implant in eyes. We're finding that all of these presumptions are not necessarily true.
At the same time, there's no question that the CTR is an important adjunct for many patients with mild or high-risk zonular problems. I encourage the use of capsular tension rings in patients who best meet the indications for use, and with attention to possible intraoperative and postoperative complications.
Dr. Ahmed is assistant professor at the University of Toronto and clinical assistant professor at the University of Utah in Salt Lake City. He holds no financial interest in any of the technologies or companies mentioned in this article. Contact him at ike.ahmed@utoronto.ca.