Evidence suggests that paraneoplastic AIR may be triggered by molecular mimicry between tumor antigens and retinal proteins. Similarly, npAIR may be triggered by molecular mimicry between retinal proteins and presumed viral or bacterial proteins. Multiple retinal proteins have been found to be antigenic; some of these are retina-specific (e.g., recoverin) and others can be found in nonretinal tissues as well (e.g., enolase). While recoverin and enolase are the most widely studied antigens in AIR, associations with autoantibodies against carbonic anhydrase, arrestin, transducin-β, TULP1, neurofilament protein, heat shock protein-70, photoreceptor-cell-specific nuclear receptor, Müller-cell-specific antigen, transient receptor potential cation channel, subfamily M, member 1 (TRPM1) and some yet-unidentified antigens have been reported.5-6 Recoverin is most commonly associated with cancer-associated retinopathy but has also been found in npAIR as well.7 These ARAs can target any retinal cell type, including photoreceptor cells, ganglion cells or bipolar cells. However, the presence of ARAs alone is not sufficient for the diagnosis of this ocular disorder, as ARAs can also be found in the serum of healthy controls.8-10
Although it is believed to be rare, the prevalence of AIR is currently unknown. The overlap of clinical features with other degenerative retinal disorders and the lack of standardized diagnostic criteria, clinical and laboratory, may be contributing to the underestimation of its prevalence.
Signs and Symptoms
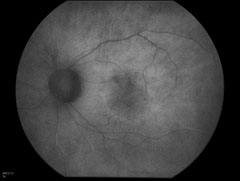
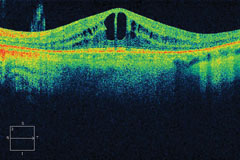
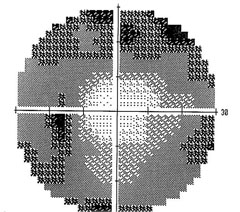
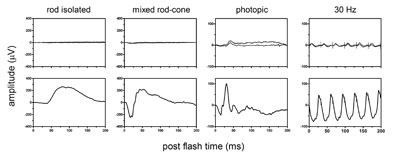
Patients with npAIR typically present with subacute vision loss, scotomas, photopsias, nyctalopia or photoaversion and dyschromatopsia. Visual acuity can be deceivingly good in the early stages. On examination, the fundus may appear unremarkable. Common clinical features in AIR patients include retinal vascular attenuation, diffuse retinal atrophy, retinal pigment epithelial changes and waxy disc pallor. AIR is usually bilateral but it can be asymmetric. Typically there are minimal or no intraocular inflammatory cells.11-14 Visual field testing shows constriction and central or paracentral scotomas, and ERG can show abnormalities in rods, cones or bipolar cell responses or a combination of these. Although rare, there may be retinal vascular leakage on angiography or cystoid macular edema on optical coherence tomography.11-12 Recent advances in imaging technology are promising. For instance, OCT and fundus autofluorescence are being investigated as tools to aid in the diagnosis of AIR, to understand its pathogenesis and to monitor disease progression.15-16
| ||||||||||||

As might be expected for an entity with no consensus in diagnosis, retrospective studies in patients with npAIR showed that clinical features vary considerably. In one study, diffuse retinal atrophy was seen in the majority of patients (83 percent) and pigment deposits in only a small proportion (13 percent), and macular edema was present in approximately half of the cases. In another study pigmentary changes were seen in approximately half of the patients and macular edema was present in only 24 percent.9,11,12,14
Differential Diagnosis
Due to the lack of definitive or standardized diagnostic criteria, the diagnosis of npAIR is difficult. Currently, the diagnosis is made based on the presence of clinical manifestations and the demonstration of serum ARAs. ARAs can be detected using Western blot, immunohistochemistry or enzyme-linked immunosorbent assay, and the majority of AIR patients may have more than one antibody.
Diagnosis is made more difficult due to the fact that the mere presence of ARAs is not diagnostic. ARAs can be found in other systemic autoimmune diseases as well as retinal degenerations, uveitis and in normal controls.18-21
Differential diagnosis of npAIR includes paraneoplastic AIR (e.g., cancer- or melanoma-associated retinopathy), white-dot syndrome spectrum disorders (particularly acute zonal occult outer retinopathy), retinal degenerative disorders (such as RP and cone-rod dystrophy), and non-infectious and infectious uveitis syndromes. RP patients can have very similar clinical features to AIR, and approximately 10 to 37 percent of patients with RP may have circulating ARAs, which makes differentiating these two entities with overlapping features very difficult.22-23 It is unclear if the antibodies in RP patients precede the onset of retinopathy or are a consequence of retinal damage. Some uveitis syndromes such as Vogt-Koyanagi Harada syndrome and sympathetic ophthalmia13,24 can also demonstrate ARAs but most of these syndromes have typical fundus findings that help differentiate them from AIR.
Because of significant implications, it is important to differentiate paraneoplastic AIR from npAIR, and an extensive investigation to rule out any malignancy should be undertaken in any patient who presents with signs and symptoms suggestive of AIR. This should include a thorough physical exam and basic laboratory investigations accompanied by an age- and gender-appropriate workup, best performed by the primary-care physician with clear communication between the ophthalmologist and primary medical team so appropriate investigations can be undertaken. Imaging with CT, MRI or PET scan should be guided by the review of systems and the patient’s individual risk factors.
Paraneoplastic retinopathies, similar to npAIR, are characterized by vision loss, photopsias, nyctalopia and scotomas with a more rapid decline. Cancer-associated retinopathy is typically associated with antirecoverin antibody, and most commonly associated with small-cell carcinoma of the lung and ERG shows involvement of cone responses.7,25-26 Melanoma-associated retinopathy occurs most commonly in patients with cutaneous melanoma and is characterized by a negative waveform on standardized full-field ERG due to reduction in b-wave amplitudes. CAR can precede the diagnosis of cancer, whereas MAR typically presents after the diagnosis of melanoma.13
|
ARAs have also been found in patients with retinal vasculitis, uveitis patients with VKH, Behçet’s disease and sympathetic ophthalmia. In patients with VKH, antibody reactivity to photoreceptors correlated with disease activity. All these syndromes are characterized by significant intraocular inflammation in addition to their unique fundus findings, making the differentiation rather unproblematic. Other rare cases of retinopathies associated with ARAs include onchocerciasis and ocular toxoplasmosis. Antibodies to retinal pigment epithelium, neural retina or photoreceptor layer have been described in these infectious retinopathies.24,29,30 Typical fundus findings in these
entities are helpful in differentiating them from AIR. In all of the aforementioned diseases, it is unclear if the antibodies preceded the retinal disease or if the immune reactivity is simply a consequence of the retinal degenerative process.
Treatment
Because of the presumed autoimmune nature of AIR, various forms of immunomodulatory approaches have been tried. However, the ambiguity in diagnosis creates an enormous challenge in the management of AIR. Immunomodulatory therapy can be considered empiric. For paraneoplastic retinopathies, decreasing tumor burden using surgery, chemotherapy or radiation, as applicable, is the best approach. Common approaches to both para- and non-paraneoplastic AIR include systemic or local corticosteroids, intravenous immunoglobulin or plasmapheresis.
| |||||||||||||||||||||
|
| |||||||||||||||||||||
|
In a cohort of 24 nonparaneoplastic AIR patients who received therapy with various combinations of prednisone, cyclosporine, azathioprine, mycophenolate mofetil, periocular or intravitreal steroid injections, 15 of the 24 showed varying degrees of improvement in visual acuity or visual field, and CME improved in almost half of the patients. Decrease in ARAs following treatment may be seen in some cases,11,24,33 however clinical significance of this finding is unclear.
In summary, there are currently no clear parameters to guide treatment and no clear indicators for prognosis. Whether changes in autoantibody levels correlate with clinical improvement is still unclear. The response to treatment is very variable, with more favorable results achieved in paraneoplastic retinopathy, particularly CAR, with a combination of chemotherapy and immunosuppression. Whether an earlier attempt to treat with immunosuppression in npAIR would be more beneficial is not known. Early treatment attempts are limited by lack of sensitive and specific assays and more definitive clinical criteria. Additional studies are needed to identify the specificity and pathogenicity of ARAs and the appropriate treatment. REVIEW
Mr. Grange is a medical student at the University of California, San Diego, who, as a participant in the National Institutes of Health Medical Research Scholars Program, is conducting clinical research with the Ocular Immunology Laboratory of the National Eye Institute. Dr. Dalal is a uveitis and ocular immunology fellow at the NEI. Dr. Sen is the director of the Uveitis and Ocular Immunology Fellowship Program at the NEI with a joint appointment as associate clinical professor with the Department of Ophthalmology at the George Washington University. Correspondence should be addressed to Dr. Sen at: senh@nei.nih.gov.
This work was supported by the NEI Intramural Research Program and the NIH MRSP, a public-private partnership supported jointly by the NIH and generous contributions to the Foundation for the NIH from Pfizer, the Leona M. and Harry B. Helmsley Charitable Trust, and the Howard Hughes Medical Institute, as well as other private donors. For a complete list, please visit the Foundation website at fnih.org.
1. Adamus G, Webb S, Shiraga S, et al. Anti-recoverin antibodies induce an increase in intracellular calcium, leading to apoptosis in retinal cells. J Autoimmun 2006;26:146-53.
2. Adamus G, Machnicki M, Elerding H, et al. Antibodies to recoverin induce apoptosis of photoreceptor and bipolar cells in vivo. J Autoimmun 1998;11:523-33.
3. Sawyer RA, Selhorst JB, Zimmerman LE, et al. Blindness caused by photoreceptor degeneration as a remote effect of cancer. Am J Ophthalmol 1976;81:606-13.
4. Klingele TG, Burde RM, Rappazzo JA, et al. Paraneoplastic retinopathy. J Clin Neuroophthalmol 1984;4(4):239-45.
5. Forooghian F, Macdonald IM, Heckenlively JR, et al. The need for standardization of antiretinal antibody detection and measurement. Am J Ophthalmol 2008;146:489-95.
6. Kondo M, Sanuki R, Ueno S, et al. Identification of autoantibodies against TRPM1 in patients with paraneoplastic retinopathy associated with ON bipolar cell dysfunction. PLoS One 2011;6:e19911.
7. Whitcup SM, Vistica BP, Milam AH, et al. Recoverin-associated retinopathy: A clinically and immunologically distinctive disease. Am J Ophthalmol 1998;126:230-37.
8. Polans AS, Witkowska D, Haley T, et al. Recoverin, a photoreceptor-specific calcium-binding protein, is expressed by the tumor of a patient with cancer-associated retinopathy. Proc Natl Acad Sci USA 1995;92:9176-80.
9. Weleber RG, Watzke RC, Shults WT, et al. Clinical and electrophysiologic characterization of paraneoplastic and autoimmune retinopathies associated with antienolase antibodies. Am J Ophthalmol 2005;139(5):780-94.
10. Ren G, Adamus G. Cellular targets of anti-alpha-enolase autoantibodies of patients with autoimmune retinopathy. J Autoimmun 2004;23:161-67.
11. Ferreyra HA, Jayasundera T, Khan NW, et al. Management of autoimmune retinopathies with immunosuppression. Arch Ophthalmol 2009;127:390-97.
12. Larson TA, Gottlieb CC, Zein WM, et al. Autoimmune retinopathy: Prognosis and treatment. Invest Ophthalmol Vis Sci 2010;51:E-Abstract 6375.
13. Chan JW. Paraneoplastic retinopathies and optic neuropathies. Surv Ophthalmol 2003;48:12-38.
14. Adamus G, Ren G, Weleber RG. Autoantibodies against retinal proteins in paraneoplastic and autoimmune retinopathy. BMC Ophthalmol 2004;4:5.
15. Lima LH, et al. Hyperautofluorescent Ring in Autoimmune Retinopathy. Retina 2012; 32:1385-94.
16. Abazari A, Allam SA, Adamus G, et al. Optical Coherence Tomography Findings in Autoimmune Retinopathy. Am J Ophthalmol 2012;153:750-56.
17. Mantel I, Ramchand KV, Holder GE, et al. Macular and retinal dysfunction of unknown origin in adults with normal fundi: Evidence for an autoimmune pathophysiology. Exp Mol Pathol 2008;84(2):90-101.
18. Shin SJ, Kim BC, Kim TI, et al. Anti-alpha-enolase antibody as a serologic marker and its correlation with disease severity in intestinal Behçet’s disease. Dig Dis Sci 2011;56(3):812-18.
19. Lee JH, Cho SB, Bang D, et al. Human anti-alpha-enolase antibody in sera from patients with Behçet’s disease and rheumatologic disorders. Clin Exp Rheumatol 2009;27(2 Suppl 53):S63-66.
20. Forooghian F, Adamus G, Sproule M, et al. Enolase autoantibodies and retinal function in multiple sclerosis patients. Graefe’s Arch Clin Exp Ophthalmol 2007;245(8):1077-84.
21. Vermeulen N, Arijs I, Joossens S, et al. Anti-alpha-enolase antibodies in patients with inflammatory bowel disease. Clin Chem 2008;54(3):534-41.
22. Heckenlively JR, Ferreyra HA. Autoimmune retinopathy: A review and summary. Semin Immunopathol 2008;30:127-34.
23. Heckenlively JR, Aptsiauri N, Nusinowitz S, et al. Investigations of antiretinal antibodies in pigmentary retinopathy and other retinal degenerations. Trans Am Ophthalmol Soc 1996;94:179-200.
24. Hooks JJ, Tso MO, Detrick B. Retinopathies associated with antiretinal antibodies. Clin Diagn Lab Immunol 2001;8(5):853-58.
25. Thirkill CE, Roth AM, Keltner JL. Cancer-associated retinopathy. Arch Ophthalmol 1987;105:372-75.
26. Keltner JL, Thirkill CE. Cancer-associated retinopathy vs recoverin-associated retinopathy. Am J Ophthalmol 1998;126:296-302.
27. Fujiwara T, Imamura Y, Giovinazzo VJ, et al. Fundus autofluorescence and optical coherence tomographic findings in acute zonal occult outer retinopathy. Retina 2010;30:1206-16.
28. Yeh S, Forooghian F, Wong WT, et al. Fundus autofluorescence imaging of the white dot syndromes. Arch Ophthalmol 2010;128:46-56.
29. Ko AC, Brinton JP, Mahajan VB, et al. Seroreactivity against aqueous-soluble and detergent-soluble retinal proteins in posterior uveitis. Arch Ophthalmol 2011;129:415-20.
30. Chan, CC, Nussenblatt RB, Kim MK, et al. Immunopathology of ocular onchocerciasis. 2. Antiretinal autoantibodies in serum and ocular fluids. Ophthalmology 1987;94:439-443.
31. Sen HN, Chan CC, Caruso RC, et al. Waldenström’s macroglobulinemia-associated retinopathy. Ophthalmology 2004;111:535-39.
32. Mahdi N, Faia LJ, Goodwin J, et al. A case of autoimmune retinopathy associated with thyroid carcinoma. Ocul Imunol Inflamm. 2010;18(4):322-23.
33. Guy J, Aptsiauri N. Treatment of paraneoplastic visual loss with intravenous immunoglobulin: Report of 3 cases. Arch Ophthalmol 1999;117:471-77.


