Presentation
A 32-year-old Ecuadorian male with no significant past medical history presented to the Wills Eye Emergency Room with four days of decreased vision in his left eye. He had no other complaints. He immigrated to the United States seven years ago.
Medical History
The patient reported no medical problems. His family history and review of systems were non-contributory. He did not smoke, drank occasionally, denied any intravenous drug use, and worked as a construction worker.
Examination
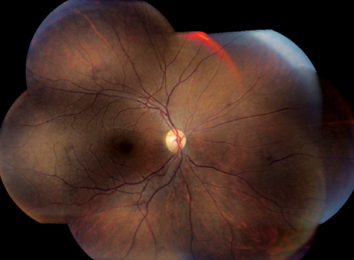
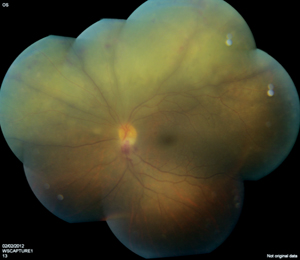
The patient’s ocular examination revealed an uncorrected visual acuity of 20/20 in the right eye and 20/40 in the left eye. Color plates were 8/8 briskly in the right eye, and 8/8 slowly in the left eye. The patient was orthophoric with full ductions and versions without diplopia or nystagmus. Visual fields were full in the right eye and decreased inferiorly in the left eye. Pupils were notable for a relative afferent pupillary defect in the left eye. External exam showed no mass, proptosis, lid lag or lid retraction. Slit lamp examination was notable for rare anterior chamber cell in the right eye and two-plus anterior chamber cell in the left eye. Two-plus anterior vitreous cell was present in the right eye and three-plus anterior vitreous cell was present in the left eye. Dilated fundus examination in the right eye showed areas of retinal pigment epithelial mottling along the arcades (See Figure 1). In the left eye, fundoscopic exam revealed multiple confluent areas of retinal whitening with perivenular areas of sparing. There was also a disc hemorrhage inferiorly, and minimal vitritis. There was no vascular sheathing.
| ||||||
What is your differential diagnosis? What further workup would you pursue?


