Presentation
A 17-year-old Caucasian male presented to the Wills Eye emergency room with a four-day history of progressive central blurring of vision in his right eye. The patient stated that he first noticed the symptoms when he was unable to read sheet music. He had no history of trauma, flashes or similar episodes in the past, but reported floaters in the right eye. A diagnosis of posterior vitreous separation had been made by his optometrist on a recent exam.
Medical History
The patient had strabismus surgery on both eyes at 18 months of age, and repeat strabismus surgery on both eyes at age 11. No records were available for review. The patient also reported a history of an "underdeveloped" optic nerve in the left eye. His medical history was significant for asthma, for which oral antihistamines were being used as well as an albuterol nebulizer. The asthma has never been treated with steroids. The patient has an allergy to sulfa-containing medications, and does not have any history of alcohol, tobacco or illicit drug use.
Examination
Visual acuity was 20/60 in the right eye and 20/25 in the left eye with no pinhole improvement. Pupil examination was within normal limits. Confrontational visual fields were full bilaterally. Extraocular motility was full in both eyes, but sensorineural examination demonstrated an alternating exotropia. Intraocular pressures were 14 mmHg in both eyes by applanation tonometry. Amsler grid testing was within normal limits on the left but showed metamorphopsia on the right. Slit-lamp examination of the lids, conjunctiva and anterior segment was within normal limits in both eyes.
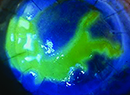
Dilated fundus examination of the right eye revealed subretinal fluid extending from the optic nerve inferiorly and temporally with sparing of the macula. The optic disc revealed a change in color along the inferonasal aspect. The fovea, vessels and periphery were within normal limits (See Figures 1 and 2). No posterior vitreous separation was observed. An OCT of the right eye was then obtained.
Dilated fundus examination of the left eye revealed a markedly asymmetric optic nerve with pigmentary changes as well as a peripheral chorioretinal scar. The vitreous, vessels and macula were within normal limits.
Diagnosis and Management
Based on the clinical presentation and examination, the patient was diagnosed with an optic pit in the right eye and an optic nerve coloboma in the left eye. Congenital optic pits and optic nerve colobomas are caused by the incomplete closure of the superior margin of the embryonic fissure. Optic pits are usually asymptomatic incidental findings in one in 11,000 individuals, with no sex or race predilection. They are usually sporadic and remain asymptomatic unless complicated by macular thickening including serous detachment, schisis and edema.
Pits can vary in size, shape and location within the disc, and may appear as a hypopigmented, gray, oval or round excavation. They are unilateral in 85 to 90 percent of cases. Typical size is 0.25 to 0.4 disc diameters. Approximately 50 percent are located on the temporal side of the disc, and one-third are central. A close proximity to the rim may increase the likelihood of serous detachments. When detachments occur, they are often delimited by an area between the disc and the arcades.
The exact mechanism by which optic nerve pits cause serous detachments is controversial. Studies on collie dogs suggest that the fluid is from the vitreous; other possibilities include leakage from marginal disc vessels and communication between the pit and subretinal space. There may be an abnormal communication between the subarachnoid space and the pit allowing cerebrospinal fluid to seep into the subretinal space.
While the diagnosis is often clinical, ancillary testing is helpful in confirming the diagnosis. OCT shows a separation between the inner and outer retina. Fluorescein angiography of optic pits is often unremarkable, but in some cases there may be late hyperfluorescence of the pit itself. Optic pits can also present with visual field defects, including an arcuate scotoma, a relative central scotoma and an enlarged blind spot.
The initial management of a symptomatic optic pit is laser photocoagulation between the area of the serous retinal detachment and the optic disc. This is thought to create a physical barrier for fluid transfer. If unsuccessful, other treatment modalities include vitrectomy with gas tamponade. Macular buckling has also been advocated. Prognosis is guarded for people presenting with vision worse than 20/70, as approximately 80 percent of these patients become 20/200 or worse.
Our patient was treated twice with approximately 100 degrees of peripapillary thermal laser, and his vision on the last follow-up appointment had improved to 20/40 in his right eye.
Dr. Ehrlich is a first-year resident. He would like to thank Dr. William Tasman for his assistance with this case.
Brown GC, Shields JA, Patty BE, Goldberg RE. Congenital pits of the optic nerve head. Experimental studies in collie dogs. Arch Ophthalmol 1979;97:1341-4.
Kuhn F, Kover F, Szabo I, Mester V. Intracranial migration of silicone oil from an eye with optic pit. Graefe's Arch Clin & Exp Ophthalmol 2006;244:1360-2.
Lincoff H, Lopez R, Kreissig I, et al. Retinoschisis associated with optic nerve pits. Arch Ophthalmol 1988;106:61-67.