When diagnosing glaucoma or monitoring its progression, doctors rely on the appearance of the disc, measures of retinal nerve fiber layer thickness and visual fields. However, other disorders of the optic nerve can also produce visual field findings, nerve fiber layer loss and disc appearance that can mimic glaucoma.
Unfortunately, a misdiagnosis can have serious consequences, not just for the patient’s vision but for the patient’s overall health and well-being. Here, I’ll review some alternative pathologies that can be misleading and share some illustrative case histories. Then, I’ll suggest a few strategies that can help ensure your diagnosis is accurate.
Optic Red Herrings
Conditions that can be mistaken for glaucoma include compressive or infiltrative lesions of the optic nerve, previous ischemic optic neuropathy (both arteritic and non-arteritic), congenital and hereditary optic neuropathies, post-traumatic optic neuropathy and inflammatory and demyelinating optic neuritis. Most cases in the compressive category—intracranial mass lesions that cause optic nerve or chiasmal compression—will be pituitary adenomas, craniopharyngiomas, suprasellar aneurysms or meningiomas. Many such tumors will present in patients who are younger than the average glaucoma patient.
Patients with compressive injury may exhibit visual fields that resemble those of a glaucoma patient, with arcuate or nerve fiber bundle loss and shallow optic disc cupping. However, it is optic nerve pallor in excess of cupping, particularly of the temporal rim, that should prompt the physician to seek etiologies other than glaucoma. A vertical step in the visual field, from involvement of the junction of the optic nerve and chiasm or the chiasm itself, should also alert the clinician of possible compression or infiltration, as should a cecocentral scotoma or decreased acuity.
Previous ischemic optic neuropathy may present with nerve fiber bundle field loss if seen after the disc swelling resolves. Arteritic ischemic optic neuropathy may result in cupping resembling glaucoma, from a loss of disc substance produced by profound ischemia. However, this is usually accompanied by marked focal arterial narrowing near the disc, and the patient may give a history of acute loss of vision with headache, jaw claudication, weight loss, anorexia and fever. In non-arteritic ischemic optic neuropathy the contralateral disc may have a small cup; the involved eye may have altitudinal pallor without cupping, but with retinal arterial narrowing.
|
Other rare causes of pseudoglaucomatous optic nerve changes include late changes after methanol-toxicity and late changes in tertiary syphilis. The history is usually helpful in toxic optic neuropathy, but identification of syphilis may require laboratory testing.
Case Histories
Here are a few real-life examples of patients whose symptoms could have led to a misdiagnosis.
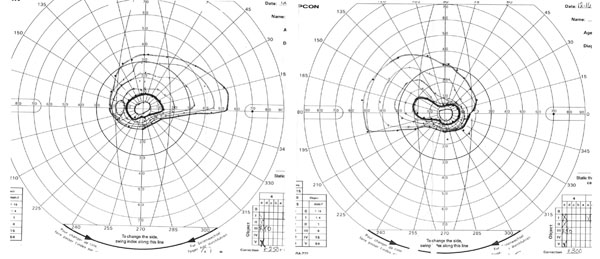
Case 1: A 55-year-old woman with diabetes and hypertension was found to have asymptomatic inferior visual field loss during a routine exam.
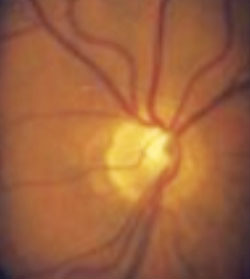
Her visual acuity, color vision and pupils were all normal; her IOPs were at the upper limit of normal. Her Goldmann visual fields showed inferior arcuate defects, often seen in glaucoma (See Figure 1A). The optic discs appeared to have abbreviated superior rims, which corresponded with the visual field defect and superior displacement of the central vessels and a superior peripapillary halo (See Figure 1B).
| ||||||||||||
This patient had superior segmental optic nerve hypoplasia, typically a consequence of maternal diabetes mellitus. This is a type of congenital optic nerve anomaly that produces a nerve fiber layer defect that can look like glaucoma. A tip-off that this is not the case is the apparent inferior visual field loss and the topless disc appearance.
Despite the dense visual field defect, the patient was unaware of it. Patients with congenital visual field loss may be described by others as “clumsy”; the defects explaining their clumsiness are often not picked up until later in life.
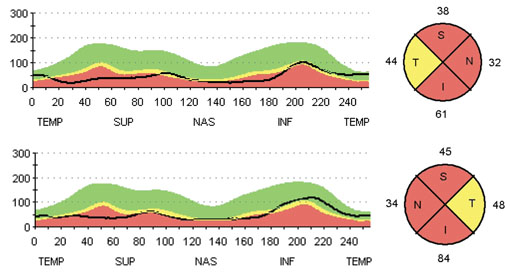
The OCT scan was also helpful in the evaluation of this patient (See Figure 1C, p. 87). It showed diffuse RNFL thinning (as opposed to thinning in just the superior area). If this patient had glaucoma, you’d expect more localized thinning corresponding to the visual field loss. In this case, the thinning was also generalized, despite being more pronounced in the superior nasal segment. Characteristically, the temporal quadrant was relatively spared, resulting in a “single peak” appearance and allowing the patient to retain good visual acuity.
In this case, the most important clues that glaucoma was not the source of the problem came from the history (i.e., the fact that the mother had diabetes and the patient was asymptomatic despite long-standing visual field loss); the appearance of the optic disc; and the OCT, which revealed widespread thinning.
Case 2. This patient was a healthy 43-year-old man, 20/60 OD, 20/80 OS, pressures 17 mmHg OU with normal central corneal thickness. Visual field testing showed bilateral cecocentral scotomas (See Figure 2A). He had slightly diminished color vision and no relative afferent pupillary defect. His vision had not changed in the recent past. He had no history of tobacco or alcohol use, and he ate well.
|
This patient had autosomal dominant optic atrophy. Similar to Leber’s hereditary optic neuropathy, end-stage dominant optic atrophy can cause disc excavation. However, unlike glaucoma, a careful observer should appreciate some optic atrophy, or temporal pallor; the rim is not going to be as pink as it would be in glaucoma. In these patients, the severity of vision loss usually peaks by adolescence and they tend to be stable for many years. The way the eye appears at adolescence is the way it will look for the remainder of the individual’s adult life. In addition, examining first-degree family members, or a history of relatives with early-onset vision loss, may aid in the diagnosis.
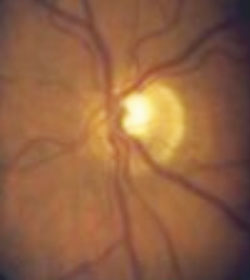
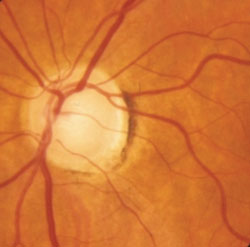
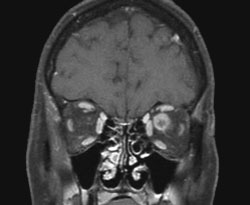
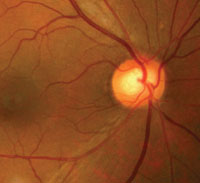
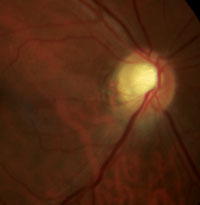
Case 3. This 42-year-old woman presented with decreased visual acuity OS. Her IOPs were normal, but she displayed a relative afferent pupillary defect and decreased color vision in the affected eye. Her visual fields indicated a left inferior altitudinal defect with a little bit of superior arcuate defect, also involving the central vision (See Figure 3B). The central foveal threshold measurement was diminished, to 36 on the right and 24 on the left. Both of her optic nerves had an increased cup-to-disc ratio. However, the left disc also had atrophy, demonstrated by relative whitening of the rim (See Figure 3A).
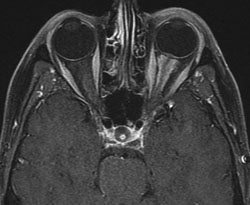
The combination of unilateral decreased visual acuity, color vision loss and optic nerve appearance required further investigation with imaging. An MRI of the orbits in this patient revealed an optic nerve sheath meningioma (See Figure 3C).
(Differential diagnosis of the MRI appearance would include other conditions such as sarcoid disease or lymphoma.) This compressive optic neuropathy may cause cupping resembling glaucoma, as well as glaucoma-like visual field defects. The difference, again, is the optic nerve appearance, pallor out of proportion to cupping, as well as color vision loss and unilateral visual acuity loss.
|

Other compressive lesions, such as pituitary adenomas and craniopharyngiomas, can lead to similar unilateral or bilateral clinical presentations. A careful clinical history and examination of the optic discs should alert the examiner to the possibility of non-glaucomatous etiologies and prompt further work-up.
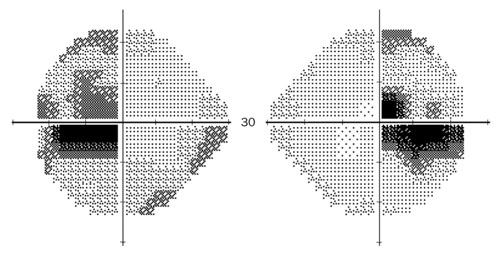
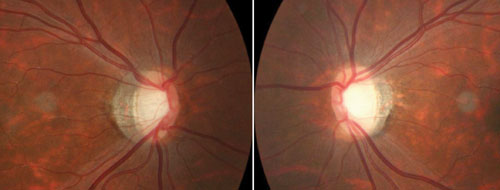
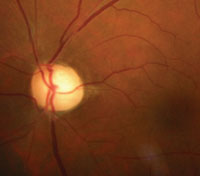
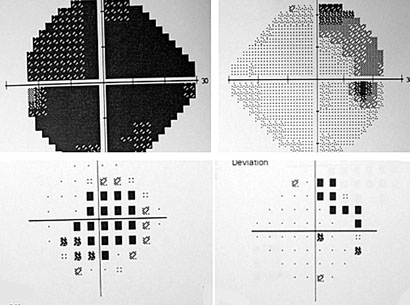
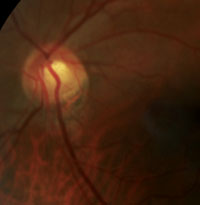
Case 4. The next case was a 48-year-old man with vision loss in the left eye (hand motion only), but 20/20 acuity in the right. He had a left relative afferent pupillary defect. The fundus examination revealed an increased cup-to-disc ratio with pallor on the left disc and a normal optic nerve on the right (See Figure 4A). The visual field showed a superior temporal defect on the right with diffuse loss on the left, also known as a junctional scotoma (See Figure 4B).
A compressive lesion in the area of the chiasm will produce such a visual field defect; compression of one optic nerve results in central vision loss and contralateral temporal fibers. Depending on the exact location of the compression, various visual field patterns can be seen. In this patient, the relatively young age, the asymmetric involvement, the visual field pattern and the optic nerve appearance prompted imaging and diagnosis of an intracranial mass lesion.
Case 5. The next patient was a 49-year-old man with elevated cholesterol. His visual acuities were 20/20 and 20/30; there was a left relative afferent pupillary defect and cecocentral visual field defect (See Figure 5A), but color vision was normal. Careful examination of the optic nerve revealed inferior swelling of the nerve fiber layer (See Figure 5B).
The patient was diagnosed with an ischemic optic neuropathy. Over time, the nerve may develop cupping, but the distinguishing feature in this situation is the development of atrophy/pallor. Increased cupping can be seen as sequelae of both arteritic and non-arteritic forms of ischemic optic neuropathy—more often the arteritic form, resulting from temporal arteritis.
Avoiding Being Fooled
A number of general strategies will help ensure that you’re not misled by pathologies that can mimic glaucoma.
| |||||||||||||||

Factors such as the family’s history of glaucoma and the patient’s age are also helpful in determining whether glaucoma is the cause. Patients with non-glaucomatous optic disc cupping tend to be younger than those with glaucoma, in part because some of them have congenital or hereditary problems.2
• Do a careful exam, and keep an open mind. Keep a high level of suspicion when the findings are not typical or what you expect—it’s possible that something else is at work. Sometimes ancillary testing, such as optical coherence tomography, may help, but mainly you have to do a thorough examination. Check color vision, scrutinize the optic disc. See whether the pattern of the visual field change that you’re seeing correlates with the appearance of the optic disc.
• Talk to the patient. You really need to do this when you first see the patient, and especially when something doesn’t make sense or isn’t adding up. What the patient has experienced may contain important clues that you can’t detect with an exam.
| |||||||||||||||
• Note the speed of progression. Some lesions will progress more quickly than you would expect glaucoma to progress—or won’t change at all.
• Don’t rely on a single piece of information. Visual fields, in particular, can produce results that look like glaucoma when other pathologies are at fault.
• When doing a visual field, leave the foveal threshold measurement turned on. This may provide useful information about central vision that isn’t obvious from simply looking at the overall field.
• Check for pallor of the optic nerve. This is probably the most important evidence that something other than glaucoma is affecting (or has affected) the optic nerve.
Large tumors in the perisellar area, pituitary adenomas or craniopharyngiomas can produce glaucoma-like optic neuropathy. Optic atrophy with pallor of the residual rim is very helpful in distinguishing these from glaucoma. One study that looked at patients with lesions that were compressing on the optic nerve in the chiasm found that pallor of the neuro-retinal rim was 94-percent specific for non-glaucomatous cupping.1
• Remember that a patient may have more than one disease. That includes having a tumor in addition to glaucoma. In such cases, it can be very challenging to try to determine what’s what and whether there’s been progression or not. A multidisciplinary approach to the patient becomes important.
• Consider the patient’s age. Studies have found that cupping in patients under the age of 50 is often due to nonglaucomatous causes.2 So if the patient is younger, don’t just assume that what you’re seeing is normal-tension glaucoma. Look for other possibilities.
• Note unexpectedly low visual acuity. Patients who have non-glaucomatous cupping of the optic nerve tend to have lower visual acuity; studies have found that vision less than 20/40 may indicate non-glaucomatous cupping associated with intracranial masses.2
Staying on the Right Track
| ||||||||||||||


The bottom line is that it’s important to keep in mind that not everything that looks like glaucoma is glaucoma. Your patient is depending on you to know the difference. REVIEW
Dr. Levin is an assistant professor of ophthalmology and visual science at Yale University and director of the ophthalmic plastic and orbital section.
1. Trobe JD, Glaser JS, Cassady J, Herschler J, Anderson DR. Nonglaucomatous excavation of the optic disc. Arch Ophthalmol 1980;98:6:1046-50.
2. Greenfield DS. Glaucomatous versus nonglaucomatous optic disc cupping: Clinical differentiation. Semin Ophthalmol 1999;14:2:95-108.



