Treatments for unhappy patients with decentered ablations or too-small optical zones haven't been developed as quickly or as fully as primary treatments for myopia, hyperopia and astigmatism. In part this is because these treatments can be hard to do, and because there's simply not as large a market for them. However, these patients are still at the refractive surgeon's ear every week, asking when they can be helped. In this, the second and final part of our look at treatments for symptomatic eyes, three refractive surgeons explain how they solve some of these patients' problems.
Tijuana surgeon and Nidek investigator Arturo Chayet, MD, has used the company's investigational software, called Customized Aspheric Treatment Zone, to treat a handful of eyes with post-refractive surgery problems.
"The software is topography- and wavefront-guided," explains Dr. Chayet. "Having topography is important, since the problems are in the cornea." The seven cases he's used it for have been patients with decentered ablations, central islands and eyes that needed their optical zones enlarged. "I see these treatments as especially powerful for decentrations," he says.
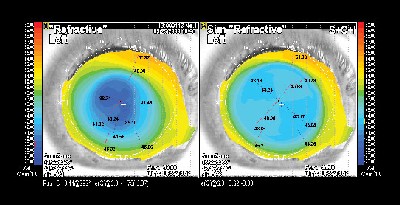 |
| Tijuana, Mexico, surgeon Arturo Chayet says the Nidek CATz system can take too-small optical zones (left) and enlarge them to a better size (right). |
The treatment process first uses Nidek's Optical Path Difference scan device to generate both a topographical and a wavefront snapshot of the patient's eye. Then, using a computer network connection or a floppy disk, that snapshot is transferred to the laser. Software called Final Fit analyzes the data and develops a treatment plan to address the patient's problem. It also indicates how much tissue the treatment will remove.
"Though it's simple, you need to play a little bit with the simulation of the results," says Dr. Chayet. "Initially, the system will suggest treatments that will take too much tissue, so we have to play around and massage the numbers to get a treatment that involves less tissue removal. We do this by changing optical zones and some ablation patterns, for example." Because these patients usually have some flap irregularity as well, Dr. Chayet says he won't hesitate to use PRK on them instead of disturbing the flap. He estimates that about half of the patients would be better suited to a surface treatment than a LASIK retreatment to help their problems.
Dr. Chayet says that the CATz software is in clinical trials, and should be available in the United States in a couple of years.
"The results in these patients are never as good as they'd be if their surgeries were perfect the first time," he says. "But it's a major help."
Bausch & Lomb's Zyoptix
University of Rochester surgeon and researcher Scott MacRae has experience with the Zyoptix system in the treatment of symptomatic patients. He says that, though the company isn't investigating an upgrade to specifically address these patients' problems, custom Zyoptix can produce satisfactory results in selected patients.
"These patients' major complaints are usually poor vision under low light conditions, halos and/or glare," explains Dr. MacRae. "There are usually decentrations or small optical zones or situations where the patient had preexisting irregular astigmatism that wasn't recognized before the original refractive procedure."
He says it's important to counsel patients with complications before you attempt to treat them so they're prepared for what could be the first of several procedures. "I usually tell the patients that they have a 66-percent chance of improvement, and that 20 percent will notice no improvement and about 10 percent will think they're slightly worse," he says. "I also make them aware that they may need one or two additional treatments to correct residual sphere or cylinder."
He says the Zyoptix approach to treating the problems will change depending on the complaint. For people with decentrations, there will primarily be large amounts of coma present, which "usually responds well to treatment," comments Dr. MacRae. Patients with relatively small optical zones usually have large amounts of spherical aberration.
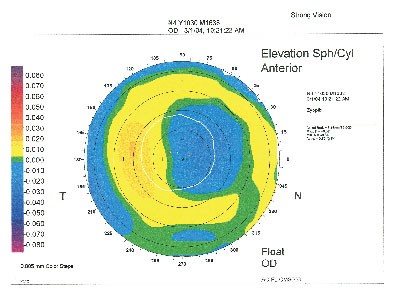 |
| A decentration after PRK made this patient's vision fuzzy, but, eight years later, a Zyoptix treatment helped sharpen his subjective vision. |
Dr. MacRae usually pulls back slightly on the sphere by 0.25 D or
0.5 D if there's some residual myopia in order to keep the patient slightly on the myopic side. "When you treat higher-order aberrations, you tend to get a little bit of hyperopia," he says.
The system will also show how much central tissue is going to be removed by the planned ablation.
Dr. MacRae says he's a little hesitant to treat central islands with the current wavefront technology, because he thinks "the next generation of wavefront sensors will be able to articulate with higher fidelity the irregularities of central islands." He says this is because the current generation of sensors, even if they have 200 to 300 lenslet spots, may only have a small number in the very center of the cornea where the central island sits.
"Symptomatic corneas present a tough area for a surgeon to work in," says Dr. MacRae. "It's challenging because there are a number of ways that a surgeon can get into trouble."
Alcon's CustomCornea
Like Zyoptix, the Alcon CustomCornea system doesn't have software specifically tailored to treat symptomatic eyes. Surgeons are making do with the custom corrections available to them to treat some patients with visual complaints.
Ronald Krueger, MD, of the Cleveland Clinic, who has treated a number of such eyes with the CustomCornea system, says you have to be careful, however. He calls these treatments "custom upgrades," which he defines as a situation in which the patient has a custom procedure to treat problems after his or her original conventional procedure. He says the upgrades can help some patients with halos, starbursts or night-vision problems postoperatively.
"These treatments are usually longer and/or deeper than conventional ones, and can potentially lead to overcorrections if there is a deep ablation depth for a relatively low refractive error," he says. As an example, he says a patient may have aberrations that are causing night-vision problems, but also only has 1 D of myopia. The system, after planning the custom ablation, may say that it will remove 50 µm or 70 µm of tissue to address the aberrations. Such a treatment may lead to an overcorrection. "If the patient's coma or spherical aberration is really high, you should be very cautious about doing that treatment," he says.
He also advises CustomCornea surgeons to use the software's plus spherical offset in nearly every upgrade case, in order to treat less sphere than what the wavefront refraction shows. "If the wavefront refraction shows
-1 D and you use a 0.5-D offset, it will only treat -0.5, in addition to all those aberrations that will take the ablation deep," he explains.
To help avoid overcorrection, he also uses a novel irrigation technique.
"Right before the treatment, after I've lifted the flap, I'll irrigate the bed with copious amounts of BSS," he says. "Then, I'll lightly wipe some of it away, leaving the stroma glistening somewhat. My plan is that the fluid may attenuate the amount of tissue removal with each pulse, avoiding excessive drying and the possibility of overcorrection."





