A 60-year-old Indian woman presented with two to three weeks of slowly progressive vision loss in her right eye. She denied redness, irritation, pain, photosensitivity, photopsias or floaters. There were no co-existing headaches, scalp pain or jaw claudication. She noted no prior ocular history, trauma or recent illnesses. Further systemic review of systems was negative.
Medical History
The patient’s past medical history was significant for type 2 diabetes mellitus and hypertension. Her most recent eye examination was greater than five years prior. Medications included sitagliptin and metformin for diabetes and lisinopril for hypertension. She reported no allergies.
Our patient moved at age 26 from India to the United States, where she currently resides. While in India she received routine medical care, including the Bacillus Calmette–Guérin (BCG) vaccine. She had no history of tobacco or alcohol use.
Examination
On initial presentation, the patient was afebrile and had stable vital signs. Her uncorrected visual acuity was 20/200 OD and 20/50¬-2 OS with no improvement on pinhole in the right eye, and improvement to 20/40 in the left eye. Pupils were equal, round and reactive to light without afferent pupillary defect, and intraocular pressures were 11 mmHg OU. Confrontational visual field testing was full to finger counting bilaterally, and extraocular muscle movements were full. Anterior segment examination revealed diffuse fine keratic precipitates in both eyes, more prominent in the right eye. The anterior chambers were deep with 2+ cell OD and 1+ cell OS. The right iris had Koeppe nodules at the iris margin; no Busacca nodules were identified. Nuclear sclerosis was moderate in the right and mild in the left eye.
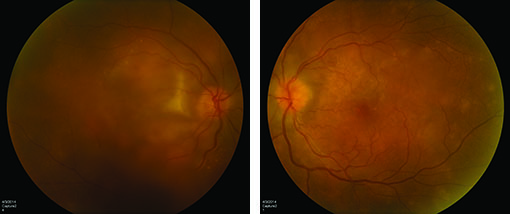
Dilated funduscopic exam revealed moderate vitreous debris OD with 1+ anterior vitreous cell and mild vitreous debris OS with no vitreous cell. Active retinitis was noted within the macula of both eyes with macular edema OD (See Figure 1). There was no optic nerve edema. Peripheral retinal examination was within normal limits.
|
What is your differential diagnosis? What further workup would you pursue?
Please click this link for diagnosis, workup, treatment and discussion.
Please click this link for diagnosis, workup, treatment and discussion.


