 |
Q: I understand that my eye exam codes are changing in January 2021. Is that true?
A: Yes. It’s a really important change—but just to the Evaluation and Management outpatient (office-based) exam codes. Those are codes 99202 to 99205 and 99212 to 99215.
Among the important changes for this 992xx exam code series is that using the history and the exam for the purposes of choosing a code are minimized, although they will remain important to documenting the reason for visits and for liability protection. Additionally, if you use inpatient hospital exam codes, those are staying the same for 2021, although they are slated for significant changes in 2022 or later.
Q: What is happening to the Medicare payments for eye exams in 2021?
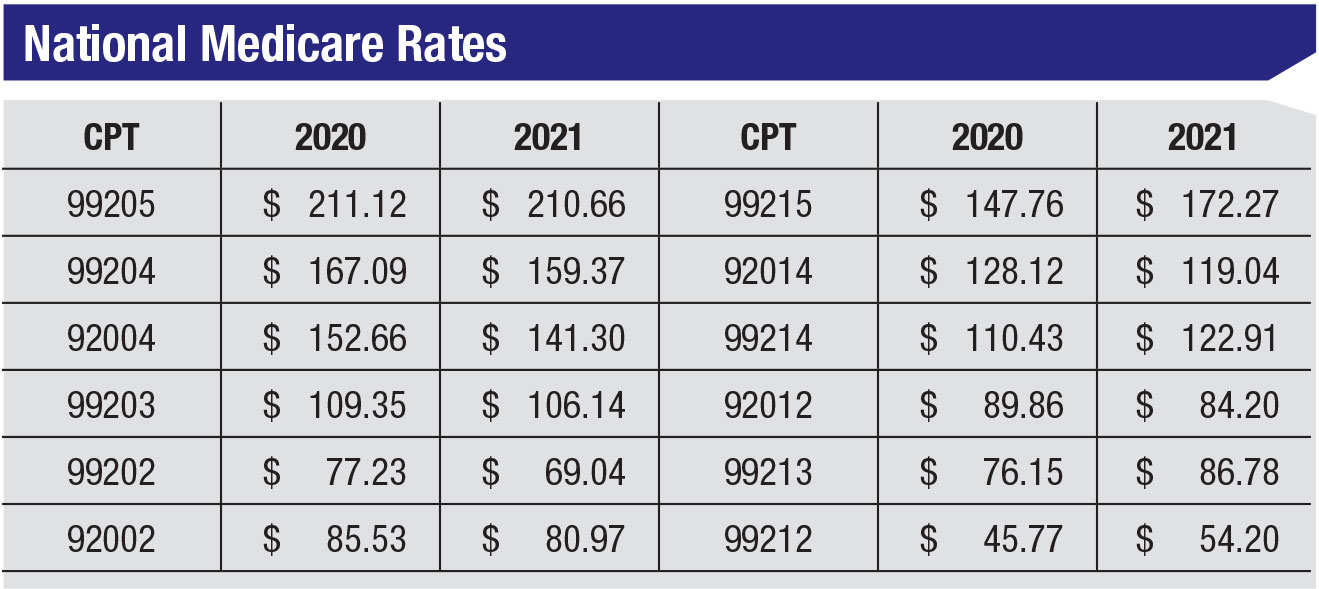
A: For medical visits, the proposed rule shows large changes in what doctors will be paid next year. It’s not final, but all of the Eye codes (92002 to 92014) are going down in value; in many cases the drop is significant. New patient E/M codes 99202 to 99205 also go down—but established patient E/M codes 99212 through 99215 are all proposed to rise significantly in payment. We should see the Final Rule and payment announcement around the first of December.
Here are the current payment amounts for 2020 and the proposed changes for 2021 (National Medicare rates):
 |
Q: That sort of decrease sounds awful. What alternatives are there?
A: Some important things to remember are that the average eye practice sees about 80 percent established patients, and only 20 percent are new patients. Although the Eye codes are all going down, an E/M code is also possible, and often will pay more in 2021 when the patient is established. Moving to E/M codes from Eye codes in a meaningful way can largely mitigate the potential revenue hit.
Q: What about the Eye exam codes? If I still get better payment on the Eye code, are the rules for using them changing?
A: The familiar Eye exam codes we commonly use: 92002; 92004; 92012; and 92014, don’t change in documentation or coding requirements and there’s no move to change them. If the eye code pays better than the E/M code that you can also code for, then stay with it.
Q: I heard the level 1 exam codes are being deleted. Is that true?
A:In 2021, E/M exam code 99201 is being deleted, but it’s of little consequence since eye doctors almost never use this code anyway.
On the established-code side, 99211 remains and is unaffected because it’s not a doctor-exam code. Payment has been and remains low even though it’s forecast to go down about $0.80 from 2020. You can still use it in the limited circumstances where it still fits.
Q: How likely is it that implementation would be delayed?
A: First, it is highly likely that this implementation will happen. A delay is very improbable. Both AMA (CPT) and Medicare support the change. Second, if it goes through, the changes will be followed by all of your other payers. Be prepared!
Q: Are the new E/M rules truly de-emphasizing the history and exam?
A: Yes. The new 2021 guidance notes that these two important components in the current 2020 rules are going to be “as medically appropriate”; the doctors decide what’s needed to support the patient and their condition at that visit. Of course, there are also important liability concerns in terms of each of these areas and you shouldn’t lose sight of that—they can’t be ignored.
|
It’s highly likely that this implementation will happen. The AMA and Medicare support it. |
Q: I heard that there are two ways to choose an E/M code in 2021. Is that true?
A: Yes. The most common way will be to use medical decision making. The other way is to use physician time. Each has been redefined in significant ways.
Q: How is coding E/M via time different?
A: In general, the time a provider spends on the exam, both face-to-face and non-face-to-face, counts if it’s not being separately reimbursed. For example, say the doctor sees a glaucoma patient and spends 25 minutes total, but five of that is looking at the billable OCT and VF done that day. Since the OCT and VF are being billed, only 20 minutes can count. Also, there are different time standards for new vs. established patients. Coding by time for a new patient begins at 15 minutes and at 10 minutes for established. Any less than those values and selection of the level of service is impossible for E/M. Eye codes don’t have a time option.
Q: If I’m not using time, and exam and history are less relevant to coding level, how is the decision-making method used?
A: There are three areas, and each uses a different methodology and guidance than the current ones use.1 It’s impossible to delve deeply into the many changes in a short article, but under the current rules, coding for a new patient is different than an established patient. In 2021 this will always be following the “2 out of 3” rule. No longer will new patients be coded as “3 out of 3.”
The three areas are 1) Problems, 2) Data, and 3) Management. For the Problems area, the number and severity of the problems, whether they are different than the last visit and their timing/frequency all play a part. Data is more complicated in the new guidance and is unlikely to be relevant to coding for eye-care providers, as we will most often use Problems and Management to arrive at a code level. Management involves how the patient is treated and the urgency of the treatments. Medical decision-making will be the more common method of choosing a code level, except for certain situations (one example is providers who do low-vision examinations). REVIEW
Mr. Larson is a senior consultant at the Corcoran Consulting Group and is based in Atlanta. He welcomes comments or questions on the topic of this month’s column. Please contact him at plarson@corcoranccg.com.
1. American Medical Association. CPT Evaluation and Management (E/M) Office or Other Outpatient (99202-99215) and Prolonged Services Code … and Guideline Changes. https://www.ama-assn.org/system/files/2019-06/cpt-office-prolonged-svs-code-changes.pdf. Accessed 10/14/2020.


