SUTURELESS VITRECTOMY, INTRODUCED by Eugene DeJuan, MD, and his colleagues about three years ago, is rapidly becoming an accepted part of the vitreoretinal surgery armamentarium. The technique relies on two concepts: 1) smaller diameter instruments and, therefore, sclerotomies; and 2) conjunctival displacement before making the transconjunctival sclerotomies so that the conjunctiva covers the sclerotomy after surgery is completed. Trocars are used to place flexible, thin-walled cannulas, resulting in 23.5-ga. sclerotomies. The cannulas are used to maintain alignment between the offset conjunctival incision and the sclerotomy and facilitate finding the small incisions when inserting tools.
Case Selection
Initially it was thought that 25-ga. sutureless vitrectomy was only going to be indicated for epimacular membranes, macular holes, vitreomacular traction, and surgery for retinal venous occlusion. Early on, many surgeons thought 25-ga. surgery was not appropriate for vitreous hemorrhages, rhegmatogenous retinal detachments, diabetic traction retinal detachments or giant breaks. Experience has shown, however, that 25-ga. surgery is ideal for vitreous hemorrhages, rhegmatogenous retinal detachments, and giant breaks, and is applicable for diabetic traction retinal detachments with modest amounts of epiretinal membranes as well. Few surgeons now believe that branch vein decompression (sheathotomy) or radial optic neurotomy are effective procedures, making 25-ga. surgery for these procedures a moot point.
Dislocated lens material (dropped nucleus) and reoperation "under" silicone require 20-ga. technique because dense membrane and silicone have too much flow resistance for small-lumen instruments. Silicone injection can be performed at the end of a 25-ga. case by enlarging one sclerotomy, which then must be sutured. (For a new development in this area, please see Expanding the Options for 25-ga. Vitrectomy in this months Feature section).
Patients with prior or anticipated glaucoma filtering procedures are ideal candidates for 25-ga. surgery. Patients with severe dry eyes, ocular surface disorders and scarred conjunctiva are excellent candidates for 25-ga. surgery, as well.
Wound Leak Issues
Postop wound leaks have always created the greatest concern about sutureless 25-ga. technology. Wound leaks can lead to hypotony resulting in choroidal detachments, bleeding, a need for vitreous volume enhancement, or reoperations to suture the wounds. Intraoperative wound leaks through the cannula can result in bleeding, vitreous prolapse with secondary vitreoretinal traction, miosis due to hypotony, or even retinal prolapse.
I initially raised the issue of conjunctival antibiotics gaining access to the vitreous cavity through unsutured sclerotomies resulting in retinal toxicity, and anecdotal reports have substantiated this concern. Dr. DeJuan has advocated allowing vitreous to plug the wounds, while I introduced the idea of using fluid-air exchange to reduce wound leaks. Many surgeons have noted the role of vitreous incarceration in 20-ga. wounds as a factor in post-vitrectomy retinal detachment. I have also emphasized that the surface tension effect of an air bubble can "seal" the sclerotomies until fibrin seals the wound, just as gas bubbles are used to "seal" retinal breaks and macular holes. In addition, I have long suggested that an air bubble in the anterior chamber is the best way to keep vitreous out of the anterior chamber and away from the wounds. Air is also an excellent way to intraoperatively "seal" wound leaks in trauma cases. I recommend removing as much peripheral vitreous as possible without lens damage in 20-ga. and 25-ga. cases.
Trocar Design Issues
The Alcon non-coring trocar is based on a modified MVR blade and requires much less insertion force than competing hypodermic needle-based, coring type designs. A prospective, consecutive clinical series that I conducted shows that the Alcon system using partial fluid air exchange demonstrates much less hypotony than other published results.
Fluidics
Ohm"s Law for fluids is directly analogous to Ohm"s Law for electricity; it teaches that pressure (gradient) equals the resistance times the flow. Resistance to flow is proportional to the fourth power of the inner diameter of the lumen. The much higher resistance of 25-ga. cutters and infusion ports was initially thought by many to be a major disadvantage. It turns out that increasing infusion pressure to about 50 mmHg while flow is occurring (dynamic state) and lowering it to about 35 mmHg (static state) when using forceps, pics, scissors or the endophotocoagulator (static state) solves the problem. The Accurus Vented Gas Forced Infusion (VGFI) system allows rapid and accurate toggling between static and dynamic infusion pressures.
The cutter has more resistance than the infusion system because of the coaxial inner needle and the cutter closing the port during the open-close cycle, thus requiring greater compensation with respect to the vacuum settings used with 20-ga. vitrectomy. I use 600 mmHg max vacuum controlled by Dual Dynamic Drive (3D) or proportional (linear) suction on the Accurus system. We have learned that fast cutting, with a 20-ga. system as well as a 25-ga., is mostly advantageous because of port-based flow limiting, which results in greater fluidic stability and therefore less retinal movement. In addition, port-based flow limiting reduces surge when dense epiretinal membrane suddenly deforms through the port, analogous to occlusion break surge in phaco procedures. Fast cutting has the added advantage of reducing vitreoretinal traction by minimizing collagen fiber travel through the port. I recommend using cutting rates from 1,200 to 1,500 cpm for all tasks and have found that core vitrectomy times are very reasonable when using 600 mmHg vacuum.
Cutter Design Options
Pneumatic disposable cutters weigh 1/14 as much as available electric cutters, thereby increasing dexterity and reducing both fatigue and flexion of the shaft. Pneumatic cutters vary (optimize) the duty cycle as a function of cutting rate, which is an advantage compared to the fixed-duty cycle of electric cutters, because of the wide range of materials properties encountered during vitrectomy (from air to perfluroctane to vitreous to dense epiretinal membrane).
Case Selection
Initially it was thought that 25-ga. sutureless vitrectomy was only going to be indicated for epimacular membranes, macular holes, vitreomacular traction, and surgery for retinal venous occlusion. Early on, many surgeons thought 25-ga. surgery was not appropriate for vitreous hemorrhages, rhegmatogenous retinal detachments, diabetic traction retinal detachments or giant breaks. Experience has shown, however, that 25-ga. surgery is ideal for vitreous hemorrhages, rhegmatogenous retinal detachments, and giant breaks, and is applicable for diabetic traction retinal detachments with modest amounts of epiretinal membranes as well. Few surgeons now believe that branch vein decompression (sheathotomy) or radial optic neurotomy are effective procedures, making 25-ga. surgery for these procedures a moot point.
|
|
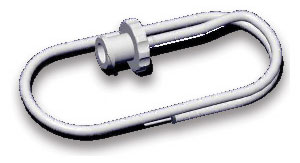
| Trocar pre-loaded with cannula as it appears just prior to insertion. The Alcon trocar is based on a non-coring, modified MVR design which requires very low insertion force and no rotation during insertion. |

Dislocated lens material (dropped nucleus) and reoperation "under" silicone require 20-ga. technique because dense membrane and silicone have too much flow resistance for small-lumen instruments. Silicone injection can be performed at the end of a 25-ga. case by enlarging one sclerotomy, which then must be sutured. (For a new development in this area, please see Expanding the Options for 25-ga. Vitrectomy in this months Feature section).
Patients with prior or anticipated glaucoma filtering procedures are ideal candidates for 25-ga. surgery. Patients with severe dry eyes, ocular surface disorders and scarred conjunctiva are excellent candidates for 25-ga. surgery, as well.
Wound Leak Issues
Postop wound leaks have always created the greatest concern about sutureless 25-ga. technology. Wound leaks can lead to hypotony resulting in choroidal detachments, bleeding, a need for vitreous volume enhancement, or reoperations to suture the wounds. Intraoperative wound leaks through the cannula can result in bleeding, vitreous prolapse with secondary vitreoretinal traction, miosis due to hypotony, or even retinal prolapse.
I initially raised the issue of conjunctival antibiotics gaining access to the vitreous cavity through unsutured sclerotomies resulting in retinal toxicity, and anecdotal reports have substantiated this concern. Dr. DeJuan has advocated allowing vitreous to plug the wounds, while I introduced the idea of using fluid-air exchange to reduce wound leaks. Many surgeons have noted the role of vitreous incarceration in 20-ga. wounds as a factor in post-vitrectomy retinal detachment. I have also emphasized that the surface tension effect of an air bubble can "seal" the sclerotomies until fibrin seals the wound, just as gas bubbles are used to "seal" retinal breaks and macular holes. In addition, I have long suggested that an air bubble in the anterior chamber is the best way to keep vitreous out of the anterior chamber and away from the wounds. Air is also an excellent way to intraoperatively "seal" wound leaks in trauma cases. I recommend removing as much peripheral vitreous as possible without lens damage in 20-ga. and 25-ga. cases.
Trocar Design Issues
The Alcon non-coring trocar is based on a modified MVR blade and requires much less insertion force than competing hypodermic needle-based, coring type designs. A prospective, consecutive clinical series that I conducted shows that the Alcon system using partial fluid air exchange demonstrates much less hypotony than other published results.
Fluidics
Ohm"s Law for fluids is directly analogous to Ohm"s Law for electricity; it teaches that pressure (gradient) equals the resistance times the flow. Resistance to flow is proportional to the fourth power of the inner diameter of the lumen. The much higher resistance of 25-ga. cutters and infusion ports was initially thought by many to be a major disadvantage. It turns out that increasing infusion pressure to about 50 mmHg while flow is occurring (dynamic state) and lowering it to about 35 mmHg (static state) when using forceps, pics, scissors or the endophotocoagulator (static state) solves the problem. The Accurus Vented Gas Forced Infusion (VGFI) system allows rapid and accurate toggling between static and dynamic infusion pressures.
|
|
|
The infusion port inserts into a cannula usually positioned at the inferior border of the lateral rectus. All three cannulas can be positioned so as to prevent damage to a filtering bleb and to best utilize displaceable conjunctiva. The port can be repositioned through different cannulas during the case to facilitate better tool access and minimize tool flexion. |
The cutter has more resistance than the infusion system because of the coaxial inner needle and the cutter closing the port during the open-close cycle, thus requiring greater compensation with respect to the vacuum settings used with 20-ga. vitrectomy. I use 600 mmHg max vacuum controlled by Dual Dynamic Drive (3D) or proportional (linear) suction on the Accurus system. We have learned that fast cutting, with a 20-ga. system as well as a 25-ga., is mostly advantageous because of port-based flow limiting, which results in greater fluidic stability and therefore less retinal movement. In addition, port-based flow limiting reduces surge when dense epiretinal membrane suddenly deforms through the port, analogous to occlusion break surge in phaco procedures. Fast cutting has the added advantage of reducing vitreoretinal traction by minimizing collagen fiber travel through the port. I recommend using cutting rates from 1,200 to 1,500 cpm for all tasks and have found that core vitrectomy times are very reasonable when using 600 mmHg vacuum.
Cutter Design Options
Pneumatic disposable cutters weigh 1/14 as much as available electric cutters, thereby increasing dexterity and reducing both fatigue and flexion of the shaft. Pneumatic cutters vary (optimize) the duty cycle as a function of cutting rate, which is an advantage compared to the fixed-duty cycle of electric cutters, because of the wide range of materials properties encountered during vitrectomy (from air to perfluroctane to vitreous to dense epiretinal membrane).
|
|



