 |
A Training Overview
In 2011, there were approximately 1,285 residency openings in India.1 This includes the three-year master of surgery and diplomate of national board programs and the two-year diploma programs. For Aravind Eye Hospitals in particular, across our six tertiary eye-care centers, about 60 residents are enrolled in our residency program each year. Candidates are required to have completed their medical school prior to residency training. Medical school training is called MBBS, short for bachelor of medicine and bachelor of surgery.
Our microsurgical training curriculum is designed keeping in mind the knowledge, skill and attitude required to become a competent surgeon. Cataract surgery knowledge is acquired through reading suggested reference books, attending a set of lectures, submitting written assignments on important topics and watching instructional videos. A set of 15 lectures is covered within the first two weeks of commencement of their training. Skill development is through teaching of surgical steps, first at the wet lab, then through simulator practice and later through surgery on patients. The third critical aspect of the mindset toward surgery is covered by clarifying expectations at the very beginning of the surgical training and at every step of learning afterward, emphasizing that patients and their outcomes always come first, ahead of the residents’ training. In terms of subspecialty training, during residency the residents pass through a rotation in various subspecialties such as retina, cornea, glaucoma, pediatric ophthalmology and oculoplastics. If they choose to undertake a fellowship, its a one- to two-year program which they undertake after the three-year residency program.
Cataract Instruction
Cataract surgical training is usually started by the fifth to eighth month of the residency program. Prior to that, the resident picks up skills in comprehensive ocular examination and preoperative evaluation of patients undergoing cataract surgery. One month is dedicated to the initial cataract surgical training, during which time the resident learns to perform extracapsular cataract extraction and manual small-incision cataract surgery. ECCE is a good technique for fostering an understanding of the anterior segment of the eye and for teaching suturing techniques. M-SICS is extremely popular in the developing world and is an effective technique employed to address cataract blindness in these settings. A dedicated trainer (medical consultant or senior anterior segment fellow) stays with the residents throughout the month. Near the end of their residency, the residents learn to perform phacoemulsification surgery.
On the first day of the month the trainee and trainer are oriented regarding the schedule and training program. In the initial few days, the residents are exposed to operation theater protocols, the central sterile supply department, patient flow in the OR, the surgical safety checklist and various local anesthetic techniques such as retrobulbar, sub-Tenon’s and facial block. In the first week they also concentrate on wet lab practice and attend the scheduled lectures.
Wet-lab training includes:
• Orientation on use of operating microscope and surgical instruments and developing hand-eye coordination.
• Practice of various suturing techniques under the operating microscope using nylon sutures and sponge.
• Use of animal eyes (goat’s eyes) and cadaver eyes (donor eyes unsuitable for corneal transplantation) are used to practice sclerocorneal tunnel construction, capsulorhexis and manual cortex aspiration using the Simcoe cannula.
• Use of the surgical simulator (EyeSi) to learn surgical concepts such as hand-eye coordination, depth perception, control of hand tremors, capsulorhexis, hydro procedures, nucleus rotation and phacoemulsification.
• Instruction in phacoemulsification machine parts, machine connections, settings and foot pedal practice.
• Instruction in phacoemulsification technique (divide and conquer) using a goat-eye model. Here, about 70 percent of the lens matter from the goat eye’s capsular bag is aspirated out and replaced with a frozen cataractous nucleus obtained from extracapsular cataract surgery. Learning phacoemulsification using this model is effective, as the surgeon is emulsifying an actual cataract.
Surgical Training
Surgical training occurs between the second and fourth week, during which time each resident typically performs five extracapsular cataract extractions followed by 12 M-SICS procedures. We emphasize appropriate patient selection, which includes patients with
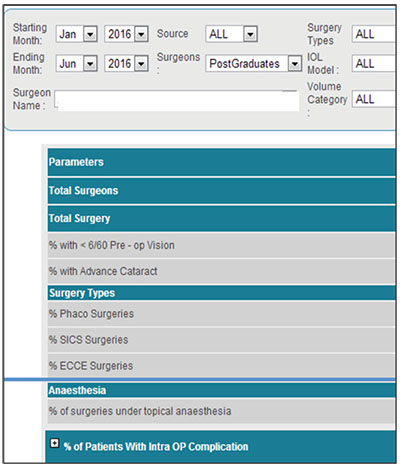 |
| Detail from Aravind’s Cataract Surgery Outcome Monitoring system. With it, residents can compare their outcomes to those of their colleagues. |
Evaluation and Feedback
The residents maintain a detailed log of the preoperative findings, surgical events and postoperative evaluation of each surgery. The consultant signs the log book on a daily basis and provides the necessary feedback. The problems faced by the resident are discussed with the trainer both immediately after surgery and during wet-lab sessions. Feedback is also provided during postoperative examination in an effort to correlate cause and effect.’The trainer uses the OSCAR (Ophthalmology Surgical Competency Assessment Rubric) tool for each surgery to assess the competence of the trainee surgeon. Besides gauging the individual surgeon’s learning curve with regard to each surgical step, the trainee surgeon also understands what s/he has to aim for in each step to become a more competent surgeon.
At the Aravind Eye Hospital, we have a data registry called the Cataract Quality Evaluation Registry. In the CATQA, information from each surgery such as demographics; preoperative, intraoperative and postoperative clinical pictures; preop and postop visual acuities; and refractive outcomes are entered into the database. This gives the residents a comprehensive view of their complication rates and visual outcomes over an extended period of time, and enables them to benchmark their performance with their peers and the rest of the institution. In addition, every quarter a senior cataract consultant reviews the data with each batch of residents and analyzes both the volume and quality of surgery performed by the residents and gives constructive feedback.
The average number of cataract surgeries performed by each resident over three years ranges from 700 to 900, most of which are M-SICS. Their complication rate is around 4 percent over the first 50 cases, decreasing gradually over the next 300 cases until it hits a level below 2 percent over the final 300 to 400.
In conclusion, a structured training curriculum with adequate wet-lab opportunities and timely feedback helps to develop residents who are confident and competent to perform quality cataract surgery. REVIEW
Dr. Aravind is chief of intraocular lens and cataract services at Aravind Eye Hospitals & Post Graduate Institute of Ophthalmology.
1. Ananthakrishnan N. Distribution of postgraduate medical seats in different disciplines: Is there rationality in decision-making? Natl Med J India. 2011;24:6:365-367.


