|
Systemic lupus erythematosus can affect virtually any organ in the body, and the American College of Rheumatology has set criteria for the diagnosis of SLE (Table 1). Although ocular manifestations are not part of the diagnostic criteria, they are common and can be observed in up to one-third of patients with SLE.5 Anterior segment findings in SLE include keratoconjunctivitis sicca, conjunctivitis, episcleritis, anterior scleritis, keratitis and iritis.5 It is important to recognize SLE-associated posterior segment disease and its association with CNS disease as a significant cause of patient morbidity.
Posterior Segment Manifestations
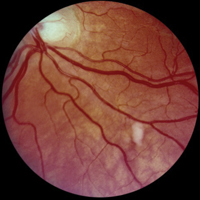
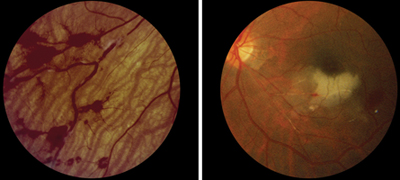
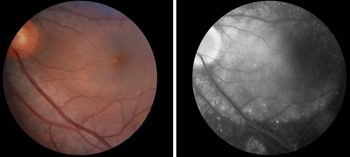
• Retinopathy. The retinopathy associated with SLE is the most common type of posterior segment finding and the risk of retinal involvement varies with disease control. It may range from 3 percent in well-controlled patients to 29 percent in patients with more active systemic disease.6,7 The most common retinal manifestation is cotton wool spots (See Figure 1), although frank phlebitis and arteritis also occur, often producing venous or arteriolar occlusion, respectively (See Figure 2, p. 43). Other manifestations may include microaneurysms, vascular tortuosity, arteriolar narrowing, retinal edema or exudates. Retinal microangiopathy associated with SLE is thought to represent immune complex-mediated vascular injury and microvascular thrombosis.8 Fortunately, most patients with mild retinopathy are at low risk for vision loss.6
| |||||||||||||||||||||||||||||
| Systemic lupus erythematosus can be diagnosed if any four or more of the 11 criteria are present serially or simultaneously, during any interval of observation. | |||||||||||||||||||||||||||||
There exists a relationship between SLE and the antiphospholipid antibody syndrome (APS). The “classical” clinical manifestations of APS, also known as Hughes’ syndrome,12 include deep venous thrombosis, cerebral arterial thrombosis, pulmonary emboli, recurrent fetal loss (predominantly in the second and third trimesters) and thrombocytopenia. Patients with at least one classical clinical manifestation of APS, along with the presence of antiphospholipid antibodies such as aCL and/or LAC antibodies in at least two samples taken three months apart, may be diagnosed with APS. Patients with APS may have SLE. However, if patients with APS do not meet the American College of Rheumatology criteria for SLE diagnosis, they can be diagnosed as having lupus-like disease (LLD) or primary APS.
The pathogenesis of antiphospholipid antibody-induced vascular thrombosis is not entirely understood, but the presence of aPL may increase plasma levels of endothelin 1 (ET-1), which could affect arterial tone and contribute to the occurrence of thrombosis.13 Severe vaso-occlusive retinopathy, including central or branch retinal artery and vein occlusion with extensive retinal capillary nonperfusion, in patients with SLE with positive aPL or primary APS has been coined Hughes’ retinopathy.14 Patients with APS generally require anticoagulation to maintain a therapeutic international normal ratio (INR) of ≥3 to have adequate prophylaxis in preventing recurrent thrombosis. Cerebrovascular disease seems to be the most associated finding seen in SLE patients with Hughes’ retinopathy,14 and proper neurological workup should be taken into consideration. Some recommend that patients with SLE and antiphospholipid-associated Hughes’ retinopathy should be started on anticoagulation in addition to treatment of the underlying rheumatological disease.14
|
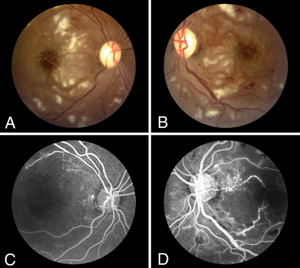
• Choroidopathy. Choroidopathy in SLE may present as multiple, serous detachments of the retinal pigmented epithelium and the neurosensory retina (See Figure 5).16-18 Visual loss can occur if the detachment affects the macula. In some cases, the subretinal fluid can progress to large, bullous exudative retinal detachments. Treatment of underlying active disease often results in resolution of the choroidopathy and associated subretinal fluid. Once the fluid resolves, the fundus may be left with a mottled appearance to the pigmented epithelium. Patients with SLE-associated choroidopathy tend to have associated systemic vascular disease either from systemic hypertension or lupus nephritis, vasculitis or a combination of these.17
|
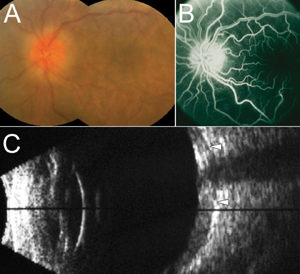
• Optic neuropathy. While the involvement of the CNS occurs in nearly 39 percent of patients with SLE,20,21 the estimated prevalence of optic neuropathy in SLE is 0.7 percent.20 Though rare, the clinical features of optic neuropathy in patients with SLE have been described, and its presentation can be highly variable. For example, a patient may present with painless vision loss, arcuate visual field defects and optic disc swelling when seen with anterior ischemic optic neuropathy, or rather with significant orbital pain associated with optic neuritis or papillitis.22 Reported ocular findings may include optic neuritis, ischemic optic neuropathy, retrobulbar optic neuropathy and optic atrophy, and optic nerve disease can affect one or both eyes.22,23 Corresponding visual field deficits, depressed visual evoked responses and afferent pupillary defects have been observed. Visual prognosis may also be variable as well, ranging from 20/20 to NLP vision depending on the extent of optic nerve damage, and this may be corticosteroid-responsive.22 The pathogenesis is thought to be related to small-vessel occlusive disease of the optic nerve, where milder cases show demyelination from mild ischemia and more severe cases exhibit significant axonal damage and necrosis.22 Of import is the association of optic nerve disease and associated CNS lesions in patients with SLE. Central nervous system lesions have been estimated to be in 54 percent of patients with lupus optic neuropathy, most commonly affecting the spinal cord.22
Treatment Options
Managing posterior segment disease typically involves the use of systemic immunosuppression with corticosteroids in the acute setting, followed by non-corticosteroid immunosuppresive agents. For severe posterior segment involvement, intravenous corticosteroid pulse therapy may be needed acutely. In some cases, local treatment with periocular corticosteroid injection may be useful. Patients with severe vaso-occlusive disease, particularly with the presence of antiphospholipid antibodies, may benefit from additional anticoagulation and/or anti-platelet treatment. In patients with profound retinal ischemia, panretinal photocoagulation and vitrectomy surgery may be needed to address complications from anterior or posterior segment neovascularization.
The Role of the Retina Specialist
Retinal specialists serve an important role in the overall care of patients with SLE. One large prospective study showed that 88 percent of SLE patients with retinopathy had active systemic disease.7 The SLE patients who developed retinopathy had a lower overall survival rate as compared to patients without retinopathy over the same time period. Moreover, active CNS involvement of lupus, a significant cause of patient morbidity, is found more often in patients with active retinopathy,7,14 retinal vaso-occlusive disease9 and optic neuropathy.22 Therefore, the presence of posterior segment findings in patients with SLE should prompt the retinal specialist to communicate with the general internist and/or rheumatologist regarding the activity and severity of their mutual patients’ disease. REVIEW
|
This work was supported in part by the Pacific Vision Foundation and the Retina Foundation. The authors have no financial interest related to this article.
Figure 3 reproduced with permission from Shein J, Shukla D, Reddy S, Yannuzzi LA, Cunningham ET Jr. Macular infarction as a presenting sign of systemic lupus erythematosus. Retina Cases & Brief Reports 2008;2:55-60.
Figure 4 reproduced with permission from Wong RW, Chan A, Johnson RN, McDonald HR, Kumar A, Gariano R, Cunningham ET Jr. Posterior scleritis in patients with systemic lupus erythematosus. Retinal Cases & Brief Reports 2010;4:326-331.
1. Rahman A, Isenberg DA. Systemic lupus erythematosus. N Engl J Med 2008;358(9):929-39.
2. Danchenko N, Satia JA, Anthony MS. Epidemiology of systemic lupus erythematosus: A comparison of worldwide disease burden. Lupus 2006;15(5):308-18.
3. Johnson AE, Gordon C, Palmer RG, Bacon PA. The prevalence and incidence of systemic lupus erythematosus in Birmingham, England. Relationship to ethnicity and country of birth. Arthritis Rheum 1995;38(4):551-8.
4. D’Cruz DP, Khamashta MA, Hughes GR. Systemic lupus erythematosus. Lancet 2007;369(9561):587-96.
5. Read RW. Clinical mini-review: systemic lupus erythematosus and the eye. Ocul Immunol Inflamm 2004;12(2):87-99.
6. Klinkhoff AV, Beattie CW, Chalmers A. Retinopathy in systemic lupus erythematosus: Relationship to disease activity. Arthritis Rheum 1986;29(9):1152-6.
7. Stafford-Brady FJ, Urowitz MB, Gladman DD, Easterbrook M. Lupus retinopathy. Patterns, associations, and prognosis. Arthritis Rheum 1988;31(9):1105-10.
8. Davies JB, Rao PK. Ocular manifestations of systemic lupus erythematosus. Curr Opin Ophthalmol 2008;19(6):512-8.
9. Jabs DA, Fine SL, Hochberg MC, et al. Severe retinal vaso-occlusive disease in systemic lupus erythematous. Arch Ophthalmol 1986;104(4):558-63.
10. Shein J, Shukla D, Reddy S., et al. Macular Infarction as a Presenting Sign of Systemic Lupus Erythematosus. Retinal Cases & Brief Reports 2008;2:55-60.
11. Au A, O’Day J. Review of severe vaso-occlusive retinopathy in systemic lupus erythematosus and the antiphospholipid syndrome: associations, visual outcomes, complications and treatment. Clin Experiment Ophthalmol 2004;32(1):87-100.
12. Hughes GR. Thrombosis, abortion, cerebral disease, and the lupus anticoagulant. Br Med J (Clin Res Ed) 1983;287(6399):1088-9.
13. Atsumi T, Khamashta MA, Haworth RS, et al. Arterial disease and thrombosis in the antiphospholipid syndrome: A pathogenic role for endothelin 1. Arthritis Rheum 1998;41(5):800-7.
14. Giorgi D, Pace F, Giorgi A, et al. Retinopathy in systemic lupus erythematosus: Pathogenesis and approach to therapy. Hum Immunol 1999;60(8):688-96.
15. Wong RW, Chan A, Johnson RN, et al. Posterior Scleritis in Patients with Systemic Lupus Erythematosus. Retinal Cases & Brief Reports 2010;4:326-31.
16. Cunningham ET, Jr., Alfred PR, Irvine AR. Central serous chorioretinopathy in patients with systemic lupus erythematosus. Ophthalmology 1996;103(12):2081-90.
17. Jabs DA, Hanneken AM, Schachat AP, Fine SL. Choroidopathy in systemic lupus erythematosus. Arch Ophthalmol 1988;106(2):230-4.
18. Nguyen QD, Uy HS, Akpek EK, et al. Choroidopathy of systemic lupus erythematosus. Lupus 2000;9(4):288-98.
19. Edouard S, Douat J, Sailler L, et al. Bilateral choroidopathy in systemic lupus erythematosus. Lupus 2011;20(11):1209-10.
20. Feinglass EJ, Arnett FC, Dorsch CA, et al. Neuropsychiatric manifestations of systemic lupus erythematosus: diagnosis, clinical spectrum, and relationship to other features of the disease. Medicine (Baltimore) 1976;55(4):323-39.
21. Hochberg MC, Boyd RE, Ahearn JM, et al. Systemic lupus erythematosus: A review of clinico-laboratory features and immunogenetic markers in 150 patients with emphasis on demographic subsets. Medicine (Baltimore) 1985;64(5):285-95.
22. Jabs DA, Miller NR, Newman SA, et al. Optic neuropathy in systemic lupus erythematosus. Arch Ophthalmol 1986;104:564-8.
23. Smith CA, Pinals RS. Optic neuritis in systemic lupus erythematosus. J Rheumatol 1982;9(6):963-6.
24. Tan EM, Cohen AS, Fries JF, et al. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 1982;25(11):1271-7.


