In response to this changing landscape, doctors have attempted to create algorithms to help clinicians navigate the management process. The first algorithms, such as the International Task Force Guidelines for Dry Eye, were created about 10 years ago; however, many clinicians still are not using them. Today, several new algorithms are in the works.
Mark S. Milner, MD, FACS, an associate clinical professor at Yale University School of Medicine and a partner and cornea specialist at the Eye Center of Southern Connecticut, is participating in several dry-eye studies and will soon be publishing his own dry-eye management algorithm. He points out that dry-eye disease can be clinically challenging, for two reasons. “First of all, dry-eye signs and symptoms can be disparate,” he says. “You can have a patient with a lot of symptoms but minimal findings, or a patient with a lot of findings but minimal symptoms. Second, there’s a misconception among many ophthalmologists that dry-eye disease is simply a quantitative problem—not enough tears. In reality, it may be a tear-quality problem as well. An abnormality in any part of the tear film, including the mucin layer and the oily layer, can lead to dry eye.”
Esen Akpek, MD, a professor of ophthalmology and rheumatology at Johns Hopkins University School of Medicine and director of the Ocular Surface Disease and Dry Eye Clinic at the Wilmer Eye Institute, notes that general ophthalmologists often don’t appreciate the value of treating dry eye. “Clinicians may assume that because dry eye is not blinding, it has no implications for a patient’s vision,” she says. “In fact, any irregularity in the tear film or epithelium can decrease quality of life because it blurs vision.”
Here, five doctors with extensive experience treating dry eye share their thoughts on diagnosis, treatment and the issues surrounding the creation of a dry-eye management algorithm.
Conducting the Exam
“Dry eye is a complex topic and an inexact science,” notes Christopher J. Rapuano, MD, director of the cornea service at Wills Eye Hospital and professor of ophthalmology at Sidney Kimmel Medical College at Thomas Jefferson University in Philadelphia. “Diagnosis is largely based on the clinical exam, meaning on the symptoms and signs. Tests can be helpful in some cases, but not all.”
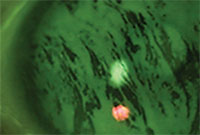 |
| Tear breakup time testing reveals rapid (<7 seconds) tear dissolution. |
Francis Mah, MD, who specializes in cornea, external disease and refractive surgery at Scripps Health System in San Diego, is a member of the American Society of Cataract and Refractive Surgery committee that is developing a new algorithm for dry-eye management. Dr. Mah says his basic exam for a dry-eye patient is straightforward. “First, I look at the tear-film meniscus to see what the tear lake looks like,” he says. “Then I do conjunctival and corneal stainings, typically with fluorescein. Lissamine green is much more sensitive for identifying conjunctival staining, but it’s become difficult to get the compounded 1% lissamine green solution, and the strips are notoriously inconsistent. Next, I do a tear-film breakup test with the fluorescein that’s still in the eye. Finally, I press on the lower eyelid to assess the consistency of the meibum.”
Stephen C. Pflugfelder, MD, a professor at Baylor College of Medicine in Houston and director of the Ocular Surface Center at Baylor’s Cullen Eye Institute, often sees complex cases—patients who have been treated elsewhere without getting relief. “We have a standardized evaluation that helps us identify problems that are less obvious,” he says. “Patients fill out two questionnaires: an ocular surface disease index questionnaire and a five-question visual analog scale measuring the frequency and severity of their irritation. Then we perform anterior segment OCT and corneal topography to look at the smoothness of the cornea. Next, we do tear osmolarity, followed by instillation of fluorescein dye to look at tear-film breakup time and corneal staining, and then lissamine green dye to look at the conjunctiva. Finally, we do a Schirmer I test without anesthesia.
“In some patients we also measure corneal sensitivity using the Cochet-Bonnet esthesiometer,” he adds. “In certain chronic dry-eye conditions such as shingles or herpes zoster, corneal sensation is reduced. The lack of nerve stimulus causes the eye to stop producing tears.”
Using the Tools
One factor adding confusion to dry-eye treatment today is the proliferation of point-of-service tests. “I think there are two reasons to do any of these tests,” says Dr. Mah. “The first is to make diagnosis and management a little bit easier for the clinician. The second reason is to reassure the patient. It’s helpful to be able to show the patient solid evidence that we’ve pinned down the problem, and that our treatment may help resolve it.”
Doctors share their thoughts about the different tools that may come in handy when diagnosing the problem:
• Dry-eye questionnaire. Dr. Mah says if a patient is not complaining of ocular surface symptoms, his technicians have the patient answer a simple questionnaire. “We use a Standard Patient Evaluation of Eye Dryness, or SPEED questionnaire,” he explains. “It’s essentially two questions that have been validated to help identify ocular surface disease. If either of the answers is positive, we proceed to perform some basic tests. One survey found that about two-thirds of patients had ocular surface complaints, even though it wasn’t the main reason for the visit.”
• Ocular surface staining. Everyone agrees that this is an essential part of any dry-eye exam. “For surface staining I like to use lissamine green and fluorescein separately,” says Dr. Akpek. “I test conjunctiva and cornea separately, because Sjögren’s-related dry eye tends to be associated with conjunctival staining; other types of dry eye such as blepharitis or evaporative-related dry eye tend to stain the cornea more. I follow the ocular surface staining scoring published in 2010 in the American Journal of Ophthalmology by John Whitcher, MD,1 because my main goal is to differentiate Sjögren’s from non-Sjögren’s dry eye and identify patients who will need prescription eye drops.”
• InflammaDry. Dr. Mah says he performs the InflammaDry test if the patient is complaining about ocular surface symptoms, or if he gets a positive result from the SPEED questionnaire. “If the InflammaDry is positive, then we follow it with the TearLab osmolarity test,” he says. “If the InflammaDry is negative, indicating that there’s little or no inflammation, I believe the osmolarity test is still important as a follow-up. In my experience, inflammation will be present whether the problem is blepharitis, meibomian gland dysfunction or an aqueous deficiency, or even if the problem is allergy or infection. So if there’s any problem at all, the InflammaDry should turn up positive. However, I would never dismiss a patient’s complaint because of a negative test.”
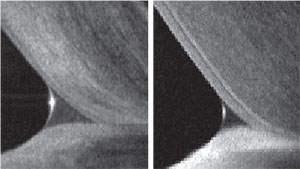 |
| Anterior segment OCT can be used to measure tear meniscus height. Left: healthy tear production. Right: Low tear production. |
Dr. Rapuano points out that this test doesn’t tell you what’s causing the inflammation. “Nevertheless, it might lead you to use steroids or an anti-inflammatory rather than punctal plugs, so it can be helpful,” he says. Dr. Pflugfelder also notes that because it’s a threshold test, it doesn’t provide a number to help grade severity.
• TearLab osmolarity test. “If the InflammaDry test reveals inflammation, the TearLab tests can help identify, at least to a small degree, whether or not it’s an evaporative problem,” says Dr. Mah. “The osmolarity test also gives us something that we can establish as a baseline, a number the patient can follow.”
“There are multiple conflicting studies regarding the effectiveness of this test,” notes Dr. Akpek. “A normal test result does not guarantee that the eye has no dry-eye disease, but an abnormal result is a good indication that there’s a problem.”
Dr. Pflugfelder says he uses it on all of his dry-eye patients, but has found it to be highly variable. “I don’t find that the test results correlate with disease severity or treatment response,” he says. “In my experience this measurement is most useful when it’s high; if it’s high, something is wrong. But a ‘normal’ reading doesn’t tell me much.”
Dr. Rapuano agrees about the variability, but says the test can still be valuable. “We’ve found that the variability is much higher in dry-eye patients than in normals,” he says. “If a patient scores 280 at one visit—which sounds great—but they’re 320 at the next visit and then 340 and then 280 again, that indicates abnormality in the tear film. Healthier eyes tend to produce similar readings at every visit. So it’s important for clinicians to understand that a one-time measurement is not necessarily the best way to use the test.”
• The Sjö test. Dr. Pflugfelder believes the Sjö test has clear value. “You’re identifying people with an autoimmune condition and the test may allow you to identify them earlier,” he says.
“It’s important to remember that one in 10 patients with clinically significant dry eye has underlying Sjögren’s,” adds Dr. Akpek. “Only a third of these patients have a diagnosis.”
• The Oculus keratograph. “The keratograph does a noninvasive tear breakup measurement and gives you a map of the areas where the tear film is breaking up more rapidly,” says Dr. Pflugfelder. “It can also measure the inferior tear meniscus height, which is among the most valuable information you can collect to determine whether patients have an aqueous-deficient or sufficient-tear dysfunction. However, we measure the tear meniscus height with anterior segment OCT.” (See example, above.)
• LipiView. “The LipiView instrument helps us assess the quality of the meibomian glands, revealing truncation of the glands and meibomian gland dropout,” explains Dr. Milner. “It also measures the lipid layer thickness and can assess how many times the patient blinks, and how many of those were partial blinks.”
“Meibomian gland imaging can be useful,” says Dr. Akpek. “It’s pretty obvious when the glands are permanently and irreversibly damaged. At this point, however, I haven’t seen enough evidence to establish a correlation between the imaging and the meibum secretion quality or the ocular surface staining scoring.”
• Topography. Dr. Pflugfelder notes that some topographers provide a measure of the smoothness of the corneal surface, which can be relevant to dry eye. “The topographer we use has validated measurements called the Klyce indices that evaluate the regularity of the rings reflected off the cornea and provide a numerical score,” he says. “People with more corneal epithelial disease from dry eye have higher scores. The Klyce Surface Regularity Index, or SRI, is valuable because it correlates with visual acuity and the severity of epithelial disease. So if someone has dry eye and the SRI is high and their vision is reduced, that would tell me that epithelial disease is probably the cause of it.”
• Schirmer test. Although this test is not reimbursable, it’s easy to perform, inexpensive and familiar to everyone, so many doctors still perform it. “This test can be helpful, especially if the result is very low or very high,” says Dr. Rapuano. “If it’s in the middle range, as many results are, it’s not that helpful to me.”
Dr. Akpek still likes to do the Schirmer test, without anesthesia. “It’s a good way to differentiate Sjögren’s-related dry eye from non-Sjögren’s-related dry eye,” she notes. Dr. Pflugfelder also does the test, but says he finds the anterior OCT measurement of the tear meniscus height to be a more valuable measure of tear volume.
Dry-eye Treatment: The Basics
Doctors largely seem to agree about the first treatment steps to take when confronted with a dry-eye patient. “We usually start with over-the-counter drops, mostly preservative-free,” says Dr. Akpek. “We’ll add a prescription anti-inflammatory eye drop after a few months if the patient isn’t getting relief, although we prescribe that right away in patients with a known underlying systemic inflammatory condition.”
“If the problem is primarily aqueous deficiency, our stepwise approach is to start with preserved tears, then switch to tears without preservatives, then to tear gels and then tear ointments,” says Dr. Rapuano. “Typically I use Restasis as the next step if the problem is chronic and not getting better. Then I use punctal plugs. However, it’s important to note that you don’t want to use punctal plugs if the patient has a significant meibomian gland problem because you can end up making unhealthy tears sit on the eye, irritating it.”
 |
“If a patient who has never used artificial tears comes in with mild dry-eye disease and no keratitis, I recommend artificial tears first,” says Dr. Milner. “I prefer nonpreserved tears, but I may start with preserved tears for reasons of cost and convenience. If the problem is more serious, I recommend nonpreserved tears because we know preservatives can exacerbate inflammation and irritation in dry-eye patients. If the patient is using artificial tears more than four or five times a day, I recommend starting Restasis or Xiidra. I don’t wait too long to add one of these, because we now believe that dry eye may be chronic and progressive; treating it earlier may help keep it from getting worse.”
The approval of Xiidra—which was found to be effective in treating both signs and symptoms of dry eye—raises the question of whether to use it or Restasis. Generally, doctors are saying it’s much too early to know when Xii-dra or Restasis might be the better option. “Restasis, topical cyclosporine, is indicated to increase tear production in patients whose tear production is presumed to be depressed due to ocular inflammation associated with keratoconjunctivitis sicca,” says Dr. Milner. “Both cyclosporine and lifitegrast are anti-inflammatory agents, and they both appear to do an excellent job.”
Dr. Milner notes that combining the drugs might also be an option. “Although there are no head-to-head studies or studies combining the two drugs, many of us in the dry-eye world believe that because they affect T-cells in different ways, they will probably be synergistic,” he says. “Combined, they may be a better option for patients who require more than one treatment. I’ve already had a number of patients on both Restasis and Xiidra for a month and a half since Xiidra’s approval, and so far, I’m seeing good results.”
Another treatment option is topical steroids. “Many of us are using steroids off-label concurrently with Restasis or Xiidra, early in treatment, to let the steroids eliminate some of the inflammation while the other drug is starting to work,” says Dr. Milner. “Of course, the risk of side effects such as glaucoma and cataract make steroids a poor choice for long-term treatment. The other caveat is to be sure to use a ‘surface steroid’ such as Lotemax or fluorometholone, which have a lower risk of causing side effects.”
Dr. Mah says he also advises dry-eye patients to take a supplement containing omega-3 fatty acids. “I’ll explain to the patient that omega-3 fatty acids are not only good for the eyes, but also for the heart to prevent stroke, and for the skin and hair,” he says. “This basic regimen is kind of a shotgun approach, but it will improve signs and symptoms in the majority of patients.”
 |
“Sometimes a bandage soft contact lens can be used to help relieve symptoms,” he adds, “but you have to be careful because dry-eye patients are at a higher risk of infection.”
Dr. Mah adds that changes in the patient’s environment might also be appropriate. “If a patient spends significant time in front of a computer, for example, it’s important to educate the patient on the connection to dry eye,” he says. “You can suggest ways to try to help reduce exacerbation such as lowering the monitor, taking short breaks or using drops during long stretches in front of the monitor.”
Mucin Deficiency & Exposure
In terms of diagnosis, most dry-eye disease can be separated into aqueous deficiency or evaporative-based. “The majority of evaporative dry eye is caused by blepharitis or meibomian gland dysfunction,” says Dr. Milner. “However, there are two other causes of evaporative dry eye that are often overlooked, and they require different treatment approaches.
“One is goblet cell deficiency, which leads to mucin deficiency,” he explains. “Mucin is critical to keeping the tears on the eye longer. Patients with a goblet cell deficiency could include anyone with cicatricial conjunctivitis, such as Stevens-Johnson Syndrome; toxic epidermal necrolysis; pemphigoid; chemical injuries; or even patients who have chronic irritation from glaucoma drops. In terms of treatment, Allergan’s Phase III study showed that cyclosporine caused a 191-percent increase in goblet cell density at six months, compared to a 13-percent in-crease for the vehicle alone.
“Another subset of evaporative dry eye is that caused by exposure, resulting from lagophthalmos, or partial blink,” he continues. “This often gets missed. You can treat for other causes, but if you miss patients who have incomplete blink, they’re going to remain dry because their lids aren’t completely covering the ocular surface. Once diagnosed, you can try having these patients tape their lids closed at night, or send them to an oculoplastics specialist if the problem is severe. In any case, even if the problem is exposure from an open eye, there may be inflammation that could be helped by cyclosporine or lifitegrast.” (Dr. Mah says another option is to have the patient use a gel or ointment at bedtime.)
Meibomian Gland Dysfunction
“If the patient has a meibomian gland problem, we prescribe warm compresses and lid scrubs first,” says Dr. Akpek. “If the patient doesn’t improve, I add a topical antibiotic, and if that isn’t sufficient I also have the patient take an oral antibiotic for several months. Lastly, I resort to tear-conserving strategies such as tear duct plugs or cauterization. Any patient who has used topical over-the-counter tears and anti-inflammatory treatment for several months and still has aqueous tear deficiency might benefit from plugs, although I wouldn’t use these as a first-line treatment in a patient with pronounced blepharitis.”
“If the problem looks like meibomian gland dysfunction, I may elect to use prescription minocycline pills instead of Restasis or Xiidra drops,” says Dr. Mah. “I usually prescribe one 50-mg pill per day, unless the patient is allergic to it, pregnant or a woman of childbearing age. I like minocycline because I currently practice in San Diego where my patients are exposed to a lot of sunlight. Doxycycline, which I often prescribed when I practiced in Pittsburgh, can cause photosensitivity; minocycline isn’t usually associated with that side effect. If the problem still hasn’t diminished after several months, I may consider using punctal plugs after Restasis or Xiidra.”
“If the problem is anterior blepharitis, that tends to be mostly infectious, so you’d want to treat that with a topical antibiotic,” says Dr. Milner. “I like to use either a topical ointment like erythromycin or bacitracin, or topical azithromycin, which I think works great. In addition to being an effective antibiotic, azithromycin has anti-inflammatory properties because it’s a macrolide, which means it can also be helpful for treating posterior blepharitis. A lot of us are also using cyclosporine off-label for posterior blepharitis with great success, and there are studies supporting this use as well.”2
 |
| Scleral lenses like the PROSE lens from the Boston Foundation for Sight allow the cornea to bathe in fluid all day. |
Dr. Rapuano says he often prescribes Medibeads, a microwavable pad you put on the eyes. “Commercial lid scrubs often work quite well,” he adds. “If the problem doesn’t improve, I have the patient use an antibiotic ointment at bedtime, either erythromycin, bacitracin or azithromycin. If that’s not enough, then we may go to oral doxycycline or minocycline, or use some mild topical steroids to get people over the hump. Omega-3 pills can also be helpful, and LipiFlow can be beneficial as well.”
When the Problem is Severe
Other treatment options can be tried when the dry-eye problem is severe and doesn’t respond to these treatments. “Moving up the ladder, you can use autologous serum eye drops, derived from the patient’s blood,” says Dr. Rapuano. “A laboratory removes the red blood cells, dilutes it and sends the serum back frozen. The patient defrosts little bottles of serum tears to use them, and some patients find them very helpful.” (For an in-depth look at the use of autologous serum, see the feature on p. 44.)
Another option is scleral lenses. “Scleral lenses sit on the sclera and bathe the cornea with fluid all day,” says Dr. Milner. “They can take dry-eye patients who have 20/200 vision and potentially return them to 20/20. This started with the PROSE lens at the Boston Foundation for Sight, but now there are clinics all over the country fitting scleral lenses. Other innovative possibilities for treating severe disease include compounded drops such as albumin, topical hormones like medroxyprogesterone and dehydroepiandrosterone, better known as DHEA. These treatments may work best for aqueous-deficient dry eye.”
If a patient has very bad mucus or filaments, Dr. Rapuano suggests trying Mucomyst (acetylcysteine), which can be made up by a compounding pharmacy. “Usually I prescribe a 10% solution four times a day,” he says. “That works well for many patients. Also, in a few patients where dry eye is severe, you can perform a small lateral tarsorrhaphy, where the eyelid is sewn closed a little on the lateral side to decrease the amount of evaporation. Patients don’t usually like it, but sometimes it really helps.”
Strategies for Success
Doctors suggest taking these steps:
• Always check your patients for dry eye. “Regardless of the reason a patient comes in to see you, you should be checking for dry eye,” says Dr. Akpek. “Treating dry eye can do a lot to improve your patient’s visual acuity and quality of life, even if the patient isn’t complaining about it.”
Dr. Rapuano adds that simply downplaying dry-eye problems is a disservice to both your patients and your practice. “As Eric Donnenfeld and others noted years ago,” he says, “if you make a dry-eye patient happy, other family members and friends are likely to come to your practice as a result. To see dry-eye treatment as just a drain on your practice is a little shortsighted.”
• Pay attention to the details of patient complaints. Dr. Mah points out that a patient’s complaint can often help with the diagnosis. “For example, if the patient is experiencing foreign body sensation in the morning, I’ll lean more toward an evaporative problem such as meibomian gland dysfunction or blepharitis,” he says. “If the symptoms are appearing late in the day or in the evening, I’m inclined to think the patient has more of an aqueous deficiency problem.”
• Be sure to gauge the severity of the problem. “At the minimum you have to have some sort of marker of severity, both in terms of symptoms and signs,” notes Dr. Pflugfelder. “You should always measure tear-film breakup time, because no matter what kind of dry eye or tear dysfunction you have, tear stability will be affected. You should also perform corneal and conjunctival staining, because those are definitely valuable. Some clinicians use osmolarity to gauge severity, but my experience has been that osmolarity isn’t trustworthy for that purpose. Others, including myself, rely on tear volume as a marker. If you can’t measure the tear meniscus height with OCT or the keratograph, the Schirmer test is an OK fallback.
“It’s also important to gauge the severity of the symptoms the patient is complaining about to act as a baseline so you can tell whether your treatment is [subjectively] causing improvement or not,” he continues. “You can do this with a dry-eye questionnaire, or by asking basic questions about situational triggers, symptoms, how often it’s a problem and how irritated the eyes are.”
• Get a sense of the impact the symptoms are having on the patient’s quality of life. “In some cases, the impact is significant to the point at which the patient is depressed and not functional,” says Dr. Pflugfelder. “If the impact is that great, you’ll probably need to go beyond the simple treatment options, and you may want to refer the patient to a dry-eye specialist.”
• Remember that the problem is frequently multifactorial. “When diagnosing, you have to decide if the problem is primarily aqueous deficiency, or it’s more evaporative, which often goes along with meibomian gland and oil problems,” says Dr. Rapuano. “The unfortunate reality is, most people have both problems. If it’s 90/10 in favor of one cause, you can treat the low-hanging fruit of the primary cause; but if it’s 50/50, then you really have to treat both causes or you’re not going to make the patient feel better.”
• Never discount a patient’s complaint. “Even if the tests are negative, we should never discount the patient’s complaint,” says Dr. Mah. “The patient knows what he or she is feeling. It’s our job to find out why they’re having the symptoms and then treat them accordingly.”
• Read dry-eye studies as they’re published. “There are multiple publications covering dry eye,” notes Dr. Akpek. “Clinicians should read the results and discussion sections, not just the abstract. Often the most important information isn’t found in the abstract.” REVIEW
Dr. Pflugfelder is a consultant for Allergan, Shire, Santen and Senju. Dr. Rapuano is a consultant for Shire and TearLab. Dr. Mah is a consultant for TearLab, Allergan and Shire. Dr. Milner is a speaker and consultant for Allergan, Shire, TearScience and Sun Pharmaceuticals and owns stock in RPS. Dr. Akpek has received institutional research support from Allergan and is currently a consultant with Shire.
1. Whitcher JP, Shiboski CH, Shiboski SC, et al. A simplified quantitative method for assessing keratoconjunctivitis sicca from the Sjögren’s Syndrome International Registry. Am J Ophthalmol 2010;149:3:405-15.
2. Perry HD, Doshi-Carnevale S, Donnenfeld ED, Solomon R, Biser SA, Bloom AH. Efficacy of commercially available topical cyclosporine A 0.05% in the treatment of meibomian gland dysfunction. Cornea 2006;25:2:171-5.


