Electronic medical records offer many benefits, such as improved documentation and efficient storage and recall of past data. However, as with most things, physicians say there’s some room for improvement in their records systems. In this article, doctors are given a platform to not only discuss their EHR gripes but also address the “wish-list” items they’d like to see included or improved upon in future EHR systems.
EHR Issues
The advent of EHRs changed the way physicians document patient interactions and, in the process, also changed those interactions. Though EHR innovations have had a positive influence on some aspects of care, Jamie Wells, MD, FAAP, a board-certified physician and director of medicine at the American Council on Science and Health, a “pro-science consumer advocacy organization,” says this isn’t necessarily so in all cases. “EHR disrupts medical practice, and it hasn’t been a positive disruptor,” she says. Claiming that the dawn of EHR was the catalyst that caused the coding and billing industry to quickly grow, Dr. Wells says this has consequently shifted attention from what she feels should be the highest priority in the medical field: the doctor-patient relationship. “You’re creating a new industry that adds third party diversion from the doctor-patient relationship, which just erodes it,” she contends.
• Preserving the doctor-patient relationship. Doctors say it’s crucial to maintain rapport with the patient, even if having the EHR system in the exam lane makes it more challenging.
Andrew Iwach, MD, executive director of the Glaucoma Center of San Francisco and board chair for the Glaucoma Research Foundation, says that when it comes to quality of care, the primary concern is the patient-doctor interaction. “My job is, number one, patient quality of care and happiness, and number two, keeping doctors happy,” he says. “We’re looking at the patient experience and how the value of our practice is perceived beyond the technical skills that we have. Patients appreciate me looking them in the eye versus looking at a terminal.” Dr. Wells agrees that understanding the patient dialogue can be as valuable, if not more valuable, than structured data. “Being a phenomenal physician vs. being a so-so one, involves utilizing not just your expertise, knowledge and experience but also skills of observation,” she says. “Your sense of vision, smell, and hearing in combination with your assessment of body language, and the patient’s facial affect can optimize diagnosis.”
Though EHR has brought new levels of efficiency and documentation to medical practice, some doctors say the need to enter data during patient interactions can put some distance between the ophthalmologist and the patient. Dr. Wells explains, “A busy practitioner has a limited amount of time, and everything that co-ops an office visit erodes the capacity to have an informed discussion or a healing conversation,” she says. “It’s crucial to watch [patients] as they answer so you can understand their state of mind, and if your head is in a computer screen, you can entirely miss the nuances of a conversation.”
Michael F. Chiang, MD, the Knowles professor of ophthalmology and medical informatics, as well as clinical epidemiology, at Oregon Health and Science University, and associate director of the OHSU Casey Eye Institute, says, “Most EHRs require the physician to direct attention toward a desktop computer—which may detract from patient-doctor communication.” However, the integration of EHR doesn’t always take attention away from the patient. Dr. Chiang says that the degree to which an EHR detracts from this interaction can depend on the specific doctor.
Michele Lim, MD, professor of ophthalmology, vice chair and medical director at the University of California-Davis Eye Center, agrees, adding that the range of doctor aptitude is pretty wide on this count. “It depends on how the doctor integrates the EHR or computer when they’re seeing a patient,” she says. “There are two ends of the spectrum: On the good side, a lot of doctors have learned to preface the visit by communicating that they’re going to take a moment to type their thoughts and background information into the computer. Then, they turn back toward the patient and talk to him or her while making eye contact, which is very acceptable.
“The other end of the spectrum would be a doctor who’s busy or in a rush,” she adds. “There are so many things to document and, usually, the computer is positioned so that your back is to the patient, which can make him or her feel like you aren’t paying attention.”
Dr. Iwach agrees that a lot of it is intuitive, based on the doctor’s feel for the interaction. “Technology is wonderful,” he says, “but it has to be implemented at the right time.” He says that understanding whether the patient is being helped is what counts, and he urges doctors to ask themselves if the way they’re using the EHR system is really helping patients.
• System issues. When it comes to EHR, there are many different systems and setups available. However, physicians say that the issues that consistently crop up usually involve “box checking” and “alarm fatigue.”
Though many physicians got into medicine for similar reasons, Dr. Wells says, nobody goes into medicine intending to check boxes. “The majority of people go into medicine for human interaction and to help people,” she says.
Dr. Chiang says that box checking may contribute to a weakening of the patient’s ability to convey important details about her complaint; the traditional patient dialogue is often being replaced by check-boxes and pre-populated text phrases, he says. Dr. Wells says that just checking a box doesn’t compel a patient to share her story. “There are many of these yes/no boxes and just checking them may not stimulate the memory of a patient interaction that would allow you to recall a certain piece of relevant information,” she says.
Some doctors are also suffering from “alarm fatigue.” Michael Boland MD, PhD, associate professor at Wilmer Eye and Health Sciences Informatics, director of information technology and residency program director at Johns Hopkins’ Wilmer Eye Institute, says alarm fatigue occurs when the EHR’s system alerts begin piling up as the physician checks boxes during the exam and history. “If you don’t pay careful attention to [reminders and pop-ups], you end up with way too many alerts for medications that don’t really make sense or apply,” he says.
Dr. Lim has thoughts on what could be behind some of the alarm-fatigue irritation. She says that some doctors are aggravated by EHR regulations, requirements and objectives set forth by the Meaningful Use program—the federal incentive for EHR adoption—which can contribute to the entering of unnecessary information. “[There’s a] feeling that EHR designers are designing toward fulfilling these regulations more than they’re trying to meet the needs of actual clinicians,” she says. Dr. Wells acknowledges that while pop-up reminders are well-intended, they can be frustrating and create unnecessary steps that shift the physician’s focus to non-clinical tasks.
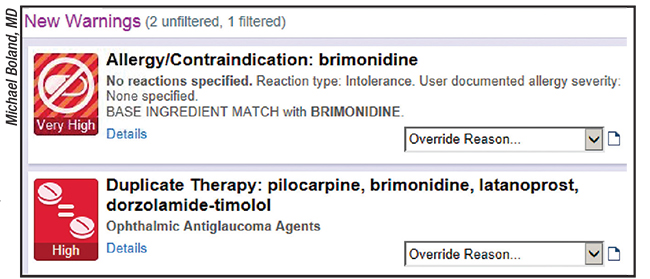 |
| Some doctors are suffering from “alarm fatigue.” Here, EHR is displaying two warnings. Wilmer’s Michael Boland, MD, says the top one is relevant (an allergy to a medication being prescribed) but the bottom one is less so (alerting Dr. Boland that the patient is on duplicate therapy for glaucoma). |
Dr. Boland says you can minimize alarm fatigue by taking the time to correctly implement an EHR system and ensure it’s customized to work as smoothly as possible. “In general, the more time you’re spending entering data, the less time you’re spending interacting with patients,” he says. To minimize alarms and reminders and make it easier to document what’s necessary without having to take as much time away from the doctor-patient relationship, Dr. Boland suggests purposefully specifying the desired workflows and designing how the EHR will implement them before configuring the system. “We have a small group at Johns Hopkins Medicine whose job is to review and approve all such decision-support tools before they can be implemented in EHR,” he says. “The design and build is done by our internal EHR team, but the vendor can help if the team runs into trouble with a particular project.
“If you don’t get the system designed to satisfy your particular requirements, you’re probably not going to be happy with it later,” Dr. Boland adds. He says that having someone internal who’s able to sit down and discuss design steps to improve a practice’s current workflow is crucial. “This job is best done by someone with both clinical and EHR/IT experience,” he says. “Such people aren’t common, so it may require sending someone from the practice to be trained on EHR configuration so they can translate between the clinical and IT worlds.” In Dr. Boland’s case, he filled this role.
Having an EHR team that works to customize parts of the EHR system, such as which drug interactions will pop an alarm, can decrease alarm fatigue Dr. Boland says. “We, as an institution, have been pretty meticulous about trying to minimize [alarm fatigue],” he says. “You want to make sure you’re only showing very-high-importance alerts; otherwise people just ignore them.”
Dr. Boland feels that some doctors are better off with EHRs and some are worse off, but that it’s related to the amount of time taken to adapt the system to their desired workflow. “If you don’t take the time to understand what will work best in your practice, [EHR] may not be equipped with the right set of processes for you, and you either end up trying to recreate a paper-based workflow using an electronic system—which isn’t a good use of it—or you try to take an out-of-the-box electronic system and wedge it into your practice,” he says.
• Data errors. Dr. Iwach says there are other issues associated with EHR beyond the changing doctor-patient interaction. He says the process of collecting data includes a lot of cut-and-paste that could contribute to errors.
“EHRs allow you to use a lot of templates, copy-forwards and shortcuts,” Dr. Lim says. “People aren’t editing the information they copy forward, so outdated data that isn’t valid anymore makes it into your current notes, which is where errors come from.” Dr. Chiang adds that reviewing everything within a short patient encounter is often difficult, due to EHRs containing so much—often redundant—data. “Findings can be imported, so it may be difficult to know exactly what occurred in the office visit,” he says.
Users say this process can cause some confusion. “Once something is written incorrectly in your record, it can follow you forever,” Dr. Wells says.
In terms of treatment options, Dr. Chiang says critical findings can be missed in long EHR notes containing standard pre-populated text (e.g., “copy-forward” and “all-normal” functions in the EHR system). “You end up with a bunch of notes you can’t trust, and you have to be very careful,” Dr. Lim adds. She says that errors can go unnoticed—or worse, a doctor could read a note containing a mistake and come to the wrong conclusion.
Dr. Wells says that a ripple effect can take place because physicians sometimes make decisions based on what’s in a record. As a member of the claims committee for the Ophthalmic Mutual Insurance Company, Dr. Iwach says one problem with medical errors is that when there’s litigation, professionals turn to the medical record because it’s regarded as the legal record of what happened. “You add a whole additional level of complexity to EMR if you have a record that’s compromised, not because of any ill intent but as a result of the demand, inconvenience and busy clinical setting,” says Dr. Iwach.
To avoid errors based on the EHR data, Drs. Chiang and Lim say that education is integral. Dr. Chiang acknowledges that medical errors occurred prior to EMRs. “[Paper] charts containing old records were often unavailable, missing or illegible at the time of medical decision-making, so they didn’t provide easy communication among different providers,” he says. However, he adds that whether records are paper or digital, it still falls to the physician to provide the best care for the patient.
Dr. Lim provides a few examples of how education has helped avoid medical errors. “In my department, we talk about [avoiding medical errors] a lot, and from the time we first started using EHR to now, people are more careful in how they enter data,” she says. “You only have to be a victim of bad data once—perhaps reading someone else’s botched note—to ensure you’re careful entering your own data.”
Dr. Lim adds that using a scribe can help avoid errors, though not every practice can afford to employ one. “A few years ago we began adopting scribes and that helps get the information down a bit more pristinely,” she says. Dr. Lim says using a scribe lets the doctor-patient conversation unfold naturally, without the disruption of entering data into a computer. However Dr. Chiang urges doctors to implement scribes properly and to ensure appropriate training. He says documentation should still be reviewed by physicians, emphasizing that it shouldn’t be outsourced to scribes.
 |
| Davis Eye Center’s Lily Koo Lin, MD, finds it helpful to use a scribe, which she says can help optimize the doctor-patient interaction. |
An EHR Wish-List
Doctors acknowledge that EHR systems are becoming a fact of life, and the current systems have a lot of potential, especially in ophthalmology, which is very data-driven. With many different needs on doctor’s minds, here are a few of the top requests.
• An improved interface. In most cases, EHR interfaces attempt to mimic a paper chart, but Dr. Wells says that the ease of paper was lost in the transition to technology. To review one patient, she may have a dozen or so tabs to navigate, making her wish that there were only a few tabs, each designated for a particular use. “One for progress, one for medical testing information and one for imaging information,” she says. “That way, you wouldn’t have to sift through 30 different tabs.”
Dr. Boland agrees, emphasizing the need for computer-driven data synthesis. He says EHR should be better at showing the doctor what he needs to see, when he needs to see it. “Systems should be more context-dependent,” he says. “If I’m seeing a patient with glaucoma, I automatically want to see IOPs and visual field results, so ideally, [the system] would take advantage of the computer’s abilities in order to show me the information graphically, or in a more digestible way.”
 |
| Trying to recreate a paper-based system using EHR isn’t a good use of the technology, surgeons say. |
In general, Dr. Lim would like enhanced customization in the form of a more graphical representation. She wants the user to be able to organize information like visual fields and pressure measurements more easily; having the ability to pull together information quickly would be a big advantage. She says she essentially does that with her scribe, but in an audible way instead of visually. When referring to the advantage of being able to ask her scribe to dictate patient-specific data, like past IOL or OCT values, Dr. Lim says, “We need an Alexa for EMR!” referring to the virtual-assistance device developed by Amazon that’s capable of voice interaction and other functions that could potentially prove helpful for ophthalmologists.
• Artificial intelligence. AI could potentially be incorporated into EHR systems in many different ways, from simply helping the doctor retain patient information to actually aiding in the diagnostic process.
Dr. Boland would like to see AI-assisted documentation to help restore the doctor-patient interaction. “People would like a better way to enter data into an EMR,” he says. “[Perhaps] through natural language processing where you just talk to the patient in the exam lane and some sort of AI assistant documents the conversation for you.” Dr. Wells says that companies are starting to test this idea using AI and voice recognition.
AI may have the ability to go even further by potentially providing decision-making assistance and guidance toward possible treatment options. Dr. Lim says there’s a lot of talk surrounding this topic. She wonders if, in the future, a physician might be able to “take pieces of disparate data, like a patient’s test results, and incorporate AI to help guide him or her toward a treatment.”
• Improved interoperability. When it comes to sharing data between different EHR systems, doctors agree significant improvement is needed. Dr. Boland calls for improved data sharing. “In ophthalmology, we need standards that let us share ophthalmology-specific data with each other,” he says. “Otherwise, we’re going to be stuck with these generic systems that were designed for primary care, which doesn’t really help us in a meaningful way.”
• Ophthalmic imaging integration. It’s a big undertaking, but many doctors feel that better integration of imaging results would benefit their practice. Currently, companies employ picture archiving and communication systems. Dr. Lim says there may be workarounds to incorporate imaging, but it’s still not truly integrated. “Most ophthalmologists have to use separate systems to capture all of their imaging results and look at them; but now you’re dealing with two different systems that you have to somehow link together,” she says. Dr. Boland agrees that it’d be better if images were integrated more tightly with EHR. In particular, he’d like more vendor-neutral analysis of OCT images. “For retina folks specifically, it’s currently a big struggle because, depending on what machine they’re using, to get images of the retina they have to launch all of the vendor-specific software to do the review,” he says. “Using two or three different systems just to view the images can become cumbersome.”
• A break from EHR? Sometimes, physicians will switch EHR systems in hopes of finding one that better suits their practice. Dr. Iwach says instead of switching EHR systems, maybe it should be more socially acceptable to take a break from EHR. “I’m not saying not to use technology, but perhaps a modified use of technology,” he says. “How about ‘efficient’ medical records, instead of ‘electronic’? Maybe we utilize some paper for taking notes but then use computers, servers and scanners in conjunction to enable more efficient data collection while still promoting the doctor-patient relationship.”
Even though he hasn’t yet implemented EHR in his practice—and therefore incurs a penalty—Dr. Iwach has a background in software and computer databases that has kept him from implementing what he feels are systems that wouldn’t quite fit within his practice. With published papers on the subject going back to his residency in the 1980s, he feels it’s his background and interest in tech that has made him more of a “cautious consumer” of software. “All I suggest is that we don’t forget there are alternatives,” he says. “It may not be an option for all settings, but don’t take [waiting to implement EHR] off the list of options. I’m passionate about the topic and I want people to be able to think, ‘maybe there’s another way.’ It’s good to have a message out there that gives people permission to question technology and its timing.”
Most doctors agree that EHRs, while not perfect, have their benefits, and they hope that, with time, the systems will have more features that doctors find useful. Dr. Boland says this may be a ship that can’t be turned around. “I think EHRs are likely here to stay, so we need to acknowledge that and focus on taking the time to consider how [EHR] can be used to make workflow better,” he says. “Take control of your EHR so that it doesn’t take control of you.” REVIEW
Drs. Wells, Lim and Boland report no relevant financial disclosures. Dr. Iwach is a consultant for Bausch & Lomb and Dr. Chiang is a consultant for Novartis and an equity owner of Inteleretina.





