A 50-year-old female visitor to the United States from China presented to the neuro-ophthalmology clinic with one week of right-side periorbital and retrobulbar pain associated with blurry vision. She described the pain around her eye as a deep, dull pressure that worsened with movement of her head and eye movements.
Medical History
Her medical history was only significant for breast cancer treated 10 years prior with mastectomy and chemotherapy, without subsequent evidence of recurrence. She took no daily medications, had no medication allergies and didn’t smoke, drink alcohol or use any illicit drugs. On review of systems she denied rashes or skin changes, joint pain, arthralgias or myalgias, paresthesias or sensory changes, balance difficulties or extremity weakness.
 |
Examination
On examination her visual acuity was 20/25 OU, her pupils were equal in size and briskly reactive to light, and there was no relative afferent pupillary defect. Intraocular pressures were 18 and 16 mmHg in the right and left eye, respectively. Extraocular motility was full bilaterally, but associated with pain on the right. Color vision by Ishihara plates was within normal limits bilaterally. External examination revealed no periocular redness or swelling, and there was no relative proptosis by Hertel exophthalmetry. Anterior slit lamp examination was notable only for bilateral posterior subcapsular cataracts.
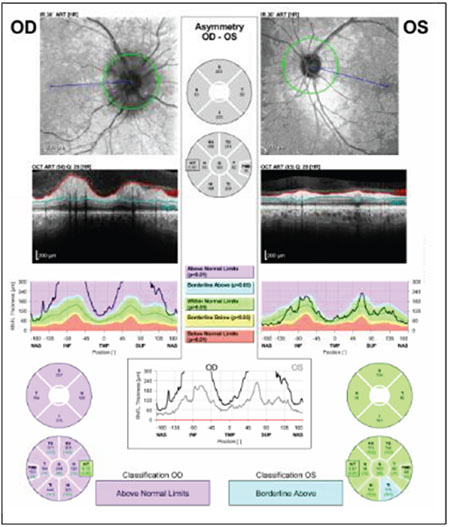
Dilated fundus examination revealed moderate, right-side disc edema without disc hemorrhages, but was otherwise normal. The left dilated fundus examination and optic nerve assessment were normal. Visual field testing by Humphrey perimeter showed blind spot enlargement in the right eye but was normal on the left. Spectral-domain OCT revealed thickening of the retinal nerve fiber layer on the right side and normal thickness on the left (Figure 1).
Click here to view the Diagnosis & Discussion.


