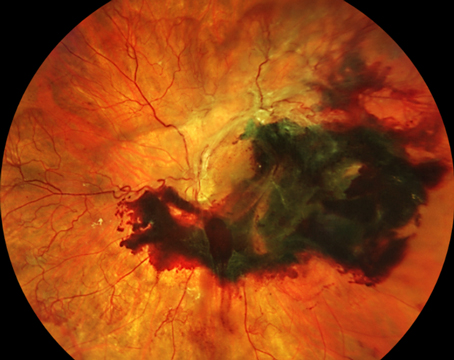
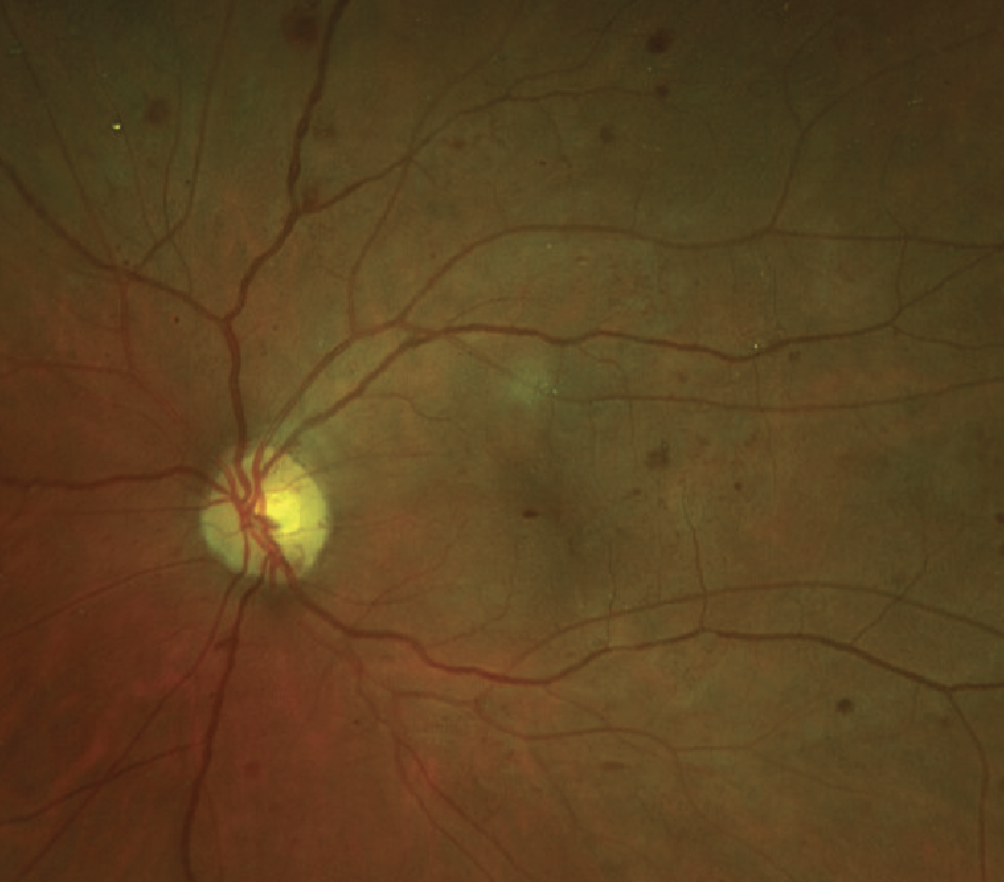
Investigators created and validated code-free automated deep learning models (autoML) for diabetic retinopathy classification from handheld-camera retinal images.
A total of 17,829 de-identified retinal images from 3,566 eyes with diabetes acquired using handheld retinal cameras in a community-based DR screening program were included.
AutoML models were generated based on previously acquired five-field (macula-centered, disc-centered, superior, inferior, temporal macula) handheld retinal images. Each individual image was labeled using the International DR and diabetic macular edema classification scale by four certified graders at a centralized reading center under oversight by a senior retina specialist. Images for model development were split 8-1-1 for training, optimization and testing to detect referable DR [(refDR), defined as moderate nonproliferative DR, or worse or any level of DME]. Internal validation was performed using a published image set from the same patient population (n=450 images from 225 eyes). External validation was performed using a publicly available retinal imaging dataset from the Asia Pacific Tele-Ophthalmology Society (n=3,662 images).
Main outcome measures included area under the precision-recall curve (AUPRC), sensitivity (SN), specificity (SP), positive predictive value (PPV) and negative predictive value (NPV), accuracy and F1 scores.
Here are some of the findings:
- RefDR was present in 17.3 percent of the training set, 39.1 percent of the internal validation sets and 48 percent of the external validation sets.
- The model’s AUPRC was 0.995 with a precision and recall of 97 percent using a score threshold of 0.5.
- Internal validation revealed the following scores:
— SN: 0.98 (CI, 0.937 to 0.995);
— SP: 0.96 (CI, 0.884 to 0.99);
— PPV: 0.98 (CI, 0.937 to 0.995);
— NPV: 0.98 (CI, 0.937 to 0.995);
— Accuracy: 0.97 (CI, 0.937 to 0.995); and
— F1: 0.96 (CI, 0.937 to 0.995).
- External validation revealed the following scores:
— SN: 0.94 (CI, 0.929 to 0.951);
— SP: 0.97 (CI, 0.957 to 0.974);
— PPV: 0.96 (CI, 0.952 to 0.971);
— NPV: 0.95 (CI, 0.935 to 0.956);
— Accuracy; 0.97 (CI, 0.935 to 0.956); and
— F1: 0.96 (CI, 0.935 to 0.956).
Investigators wrote that the findings validated the accuracy and feasibility of code-free automated machine learning models for identifying referable diabetic retinopathy developed using handheld retinal imaging in a community-based screening program. They added that the use of automated machine learning may increase access to similar models that may be adapted for specific clinical programs.
Ophthalmol Retina 2023; Mar 14. [Epub ahead of print].
Jacoba CMP, Doan D, Salongccay RP, et al.
 |
Visual Impairment after Anti-VEGF Injections
Intravitreal anti-VEGF injections are the current standard of care for treating neovascular age-related macular degeneration, but vision loss still occurs in some patients. Researchers believe that the vision loss affecting this small subgroup of patients may be related to the number of intravitreal injections they receive.
Investigators conducted a retrospective, observational study analyzing patients who experienced sudden visual decline, defined as a loss of ≥15 ETDRS letters, during anti-VEGF treatment for nAMD. A total of 1,019 eyes received treatment during the study period, with severe vision loss occurring in 15.1 percent of patients after a median of six injections. Ranibizumab was injected in 52.8 percent of cases and aflibercept in 31.9 percent. The researchers reported that functional recovery after three months was significant and showed no further improvement at six months.
The researchers also reported better visual outcomes in eyes with no substantial central macular thickness changes compared with eyes that had an increase of >20 percent or a decrease of >5 percent in thickness.
The researchers say that, to their knowledge, this is the first real-life study exploring the incidence, OCT correlation and intermediate prognosis of severe visual acuity loss during anti-VEGF treatment in patients with nAMD. They found that a ≥15 ETDRS letter loss between two consecutive intravitreal injections wasn’t unusual in patients receiving intravitreal injection treatment. Since the loss frequently occurred within nine months of diagnosis and two months after the last intravitreal injection, the physicians recommend close follow-up and a proactive regimen, at least in the first year.
Retina 2023; Mar 9. [Epub ahead of print].
Grassi MO, Monteleone G, Pozharitskiy N, et al.
Central Field Damage in Glaucomatous Eyes
Researchers characterized the relationship between deep-layer microvasculature dropout (MvD) and central visual field damage in primary open-angle glaucoma patients with and without high axial myopia, as part of a cross-sectional study.
Seventy-one eyes (49 patients) with high axial myopia and POAG and 125 non-highly myopic POAG eyes (97 patients) were enrolled. Presence, area and angular circumference of juxtapapillary MvD were evaluated on optical coherence tomography angiography B-scans and en face choroidal images.
Here are some of the findings:
- Juxtapapillary MvD was detected more often in the highly myopic POAG eyes (43 eyes, 86 percent) than in the non-highly myopic eyes (73 eyes, 61.9 percent; p=0.002).
- In eyes with MvD, the following were significantly larger in highly myopic eyes vs. non-highly myopic eyes:
— MvD area (area [0.69; CI, 0.40, 0.98]) mm2 vs. 0.31 (CI, 0.19, 0.42) mm2; p=0.011) and
— angular circumference (84.3 [CI, 62.9 to 105.8] vs. 74.5 [CI, 58.3 to 90.9]); p<0.001.
- 24-2 VF mean deviation was significantly worse in eyes with MvD compared with eyes without MvD in both groups (p<0.001).
- After adjusting for 24-2 MD VF, central visual field defects were more frequently found in eyes with MvD compared with eyes without MvD (82.7 vs. 60.9 percent; p<0.001).
- In multivariable analysis, higher intraocular pressure, worse 24-2 VF MD, longer axial length and greater MvD area and angular circumference were associated with worse 10-2 VF MD.
Researchers found microvasculature dropout was more prevalent and larger in primary open-angle glaucoma eyes with high myopia than in non-highly myopic primary open-angle glaucoma eyes. In both groups, eyes with microvasculature dropout showed worse glaucoma severity and more central VF defects.
Br J Ophthalmol 2023; Feb 20. [Epub ahead of print].
Micheletti E, El-Nimri N, Nishida T, et al.
Retinal Effects of Combined Cornea/Cataract Procedures
Scientists evaluated alterations in central retinal thickness (CRT) and their implications for visual acuity after ultrathin Descemet’s stripping automated endothelial keratoplasty (UT-DSAEK) and Descemet’s membrane endothelial keratoplasty (DMEK) combined with cataract surgery.
A total of 72 eyes of 72 patients with Fuchs’ endothelial dystrophy and cataract were included and equally randomized to UT-DSAEK or DMEK. A control group of 40 eyes of 40 patients with cataract were included for cataract surgery. All participants were examined preoperatively, as well as three and six months postoperatively.
Here are some of the findings:
- No significant differences were reported in central retinal thickness between the study groups after surgery (p=0.896).
- A significant difference in best-corrected visual acuity progression over time was found between the study groups (p<0.0001).
- Average improvements of 8.03 EDTRS after UT-DSAEK (p<0.001) and 16.77 EDTRS after DMEK (p<0.001) were found six months postoperatively.
- No significant correlation was found between the change in best-corrected visual acuity and central retinal thickness from baseline to three months postoperatively (r2<0.0001; p=0.96) and from baseline to six months postoperatively (r2=0.0053; p=0.46).
Scientists wrote that central retinal thickness wasn’t altered by ultrathin-Descemet’s stripping automated endothelial keratoplasty, Descemet’s membrane endothelial keratoplasty or cataract surgery three and six months postoperatively.
They added that the patients’ best-corrected visual acuity significantly improved three months after UT-DSAEK and six months after DMEK. The investigators didn’t find any significant correlations between the change in the subjects’ best-corrected visual acuity and their central retinal thickness postoperatively. As such, the scientists concluded that CRT alterations were comparable after UT-DSAEK, DMEK and cataract surgery.
Cornea 2023; Feb. 27. [Epub ahead of print].
Madsen M, Brok M, Anders I, et al.