Symptoms of dry eye are some of the most common complaints encountered in any ophthalmologist's clinic. As many of us are aware, there is no perfect treatment, and the patients often suffer from many exacerbating factors, such as those secondary to environment (heating, air conditioning, low humidity) and activities (computer work, reading). Though dry-eye symptoms can be significantly reduced with the use of artificial tears of varying viscosity, patients can feel burdened with the frequent use of such aqueous tear enhancers and become non-compliant. Punctal plugs can relieve some of this burden, and in this article, I'll explain how I put them to use in my practice.
Involve the Patient
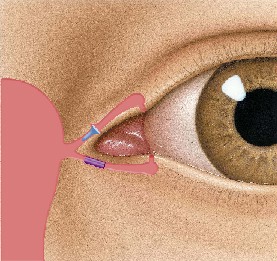
Inside the punctum, the SmartPlug shrinks in length and expands in width, adjusting itself to fit. Once in place, it becomes a virtually undetectable soft gel.
Punctal occlusion can greatly diminish dry-eye symptoms when used appropriately. Many of us are familiar with their use, but are often less certain about when to use them and which type to use. Explaining the role of punctal occlusion to the patient is important. The patient is often unaware of her own tear ducts and is fearful when doctors use the word "silicone" when discussing implants. She should not be led to believe that plugs will cure her disease, nor that they will allow her to stop using artificial tears altogether. In addition, I like to include the patient in the decision-making process and give her the option of deferring such elective measures when any risk is involved. After consideration of risks and benefits, many patients choose to use an aggressive tear regimen instead of moving forward with plugs.

Odyssey Medical"s Parasol
Varieties of Occlusion
There are a variety of ways to create punctal occlusion: temporary, semi-permanent and permanent. Temporary refers to the use of collagen plugs that dissolve in less than a week. Semi-permanent refers to the use of durable materials like silicone or thermal labile acrylic polymers. Permanent occlusion means complete closure of the punctum with thermal or laser cautery. In a hesitant patient, collagen plugs are often used as an inexpensive trial to determine whether more permanent occlusion can help.
Where to Begin
With regards to treatment, I start with only artificial tears in most cases. This approach reinforces the fact that dry-eye patients will always need surface lubricants to treat their disease and symptoms. I tell them there are more advanced options like plugs or topical cyclosporine, but because there is more risk (albeit small) and cost to them, I use those only when necessary. Then, if symptoms decrease but aren't eliminated, I consider adding punctal occlusion to the regimen. The exception to this rule for me is when there are significant exam findings that may result in serious ocular morbidity (e.g., sterile ulcers, dellen) or when rapid improvement of the ocular surface is required, as in pre- or post-LASIK patients. I generally start with bilateral lower punctal occlusion and add upper plugs only if necessary upon follow-up.
If the patient notices definite benefit with temporary occlusion, I will move to plug placement. I don't do serial temporary occlusion. If the patient notices little or no benefit, I'll still give her the option of placing semi-permanent plugs. If she has clinical findings that improve with temporary plugs, however, I'll encourage plug placement. If the semi-permanent plug spontaneously extrudes, I'll ask the patient if she believes it was helping before it came out. If she says no, I may defer replacement of the plug due to subsequent decreased retention rate (see below). When any type of plug is placed or replaced, chart documentation is important to prevent another doctor's attempt to place a plug. The location of a plug may not be immediately obvious.
 |
| The non-dissolvable Blue Opaque Herrick Lacrimal plug rests in the upper caniculus while a disposable Opaque Herrick Lacrimal Plug provides temporary occlusion in the lower; just one of several treatment combinations available to the creative ophthalmologist. |
Complications
Although simple, safe, and effective, punctal plugs are not risk-free. Documented complications include ocular discomfort and irritation, spontaneous extrusion/loss, granulomas, and canalicular migration with secondary nasolacrimal obstruction, canaliculitis, or dacryocystitis requiring surgical removal.
Another common "complication" is loss of the plug. Initial plug retention has published rates of 50 to 63 percent at six months for standard plugs. Repeat plug placement has an even lower retention rate. However, newer plug designs theoretically facilitate insertion and improve retention rate. If a patient has done well with plugs but suffers frequent loss, I will consider use of the newer SmartPlug from Medennium or permanent occlusion with cautery, as opposed to multiple repeat insertions with potential damage to surrounding tissue.
Beginning Occlusion
When is the appropriate time to begin using punctual occlusion? Again, I like to include the patient in the decision-making process. I typically recommend semi-permanent punctal occlusion with silicone plugs in both lower lids when patients are symptomatic from dry eyes despite adequate compliance with artificial tears more often than four times per day. I examine the puncta at the slit lamp to determine the ideal size, choosing the largest size possible. This process is an estimate only. If, when placing the first plug, I notice it fits too easily, I'll increase the plug size of the fellow eye by 0.1 mm.
| Choosing Punctal Occlusion |
| "Awareness of dry eye has greatly increased, and now there are better methods to treat the condition in addition to prescribing artificial tears," says Odyssey Medical's Emily Whitlow. She points to an aging America and an increase in refractive surgery and the dry eye associated with it as top reasons for growth in the punctal-plugs market. In September, Odyssey extended its line of Parasol Punctal Occluders to include an extra-small size, hoping to meet the needs of patients of every size. Whether you choose dissolvable or non-dissolvable plugs for your patient, and decide to use them for treatment over the short term, the intermediate term, or the long term, there's an abundance of plug styles and materials from which to select: |
| Eagle Vision eaglevis.com 1-800-222-7584 Offering the EaglePlug, the EagleFlexPlug, the Flow Controller and dissolvable collagen inserts. |
| FCI Ophthalmics fci-ophthalmics.com 1-800-932-4202 Offering the Ready-Set plugs, PVP Perforated plugs and dissolvable collagen inserts. |
| Lacrimedics lacrimedics.com 1-800-367-8327 The Herrick System of Occlusion Therapy features dissolvable collagen plugs, synthetic dissolvable Opaque Herrick lacrimal plugs and Blue Opaque Herrick lacrimal plugs. |
| Medennium medennium.com 1-888-727-6100 Offering the thermosensitive acrylic SmartPlug. |
| Oasis Medical oasismedical.com 1-800-528-9786 Offering silicone plugs, extended duration plugs and dissolvable collagen plugs. |
| Odyssey Medical odysseymed.com 1-888-905-7770 Featuring the Parasol Punctal Occluder system, the Plus punctal occluder, dissolvable collagen implants and the Extend absorbable synthetic punctal implants. |
| Surgical Specialties surgicalspecialties.com 1-800-523-3332 Offering the UltraPlug in three styles: extended wear synthetic absorbable plugs, collagen absorbable plugs and silicone plugs. |
| U.S. IOL usiol.com 1-800-354-7848 Offering the Occu-Flo punctum plug. |
When placing the plug, some physicians prefer to do so with the visual aid of the slit lamp, but it's easier and faster for me to simply to have the patient lean back in the exam chair under good lighting. I then look at the fit with the slit lamp prior to discharging her from clinic, telling the patient that the plugs' orientation and fit look good. This way, she is aware of the "normal" sensation of a plug.
The newer, labile plugs like SmartPlug (Medennium, Irvine, Calif.) have a slightly different method of insertion. Because the SmartPlug is a "one-size-fits-all" plug, there is no need to measure the punctum size, just inspect it for punctal patency. This also eliminates unnecessary trips to the supply room and wasting plugs that don't fit. The SmartPlug is inserted at the slit lamp to 2/3 of its length; it then contracts completely within the canaliculus. The downside of this style of plug is the fact that you can't easily monitor its presence if the patient continues to have symptoms.
Overall, I see a very high success rate with the use of punctal plugs with regards to reducing symptoms and signs of dry eye safely and effectively. Still, dry eyes tend to produce chronic symptoms. There will always be patients who continue to have symptoms despite maximum therapy with lubricants, cyclosporine, plugs, diet, environmental trials, etc. Because of these non-responders, I look forward to new developments in the ongoing research of dry eye.
Dr. Blackmon is an assistant clinical professor in the department of ophthalmology at Duke University Eye Center with a special interest in dry eyes and refractive surgery. Contact him at douglas.blackmon@duke.edu.


