The Light-Adjustable Lens from Calhoun Vision (
Creating Multifocality
To understand how a monofocal lens could be turned into a multifocal one in the eye, it helps to understand how the LAL process works.
The LAL is a silicone intraocular lens with a 6-mm optic. On the molecular level, though, the lens is only partially polymerized. It's actually a silicone matrix full of unpolymerized silicone macromers that are tied to photosensitive molecules.
Using a specific wavelength of light emitted from a slit-lamp-sized device made by Carl Zeiss Meditec, the ophthalmologist can adjust the lens power after the lens is already in the patient's eye by polymerizing the unpolymerized macromers, which induces a change in thickness in selected areas of the lens. 
Before the light reaches the LAL, it passes through a filter that shapes it to the precise spatial intensity distribution needed to create a specific power change. This distribution could involve placing more light in the periphery of the lens, the center or any place necessary to cause the change the surgeon needs. The user can adjust the power by as little as 0.25 D, and the adjustment is usually made one to four weeks postop.
The light source used with the LAL adds thickness to the lens wherever it strikes it by causing the silicone to build up in those particular regions. For example, if the LAL patient has a hyperopic refractive error after cataract surgery, then the lens doesn't have enough power. To adjust this, the surgeon shines a light pattern with more intensity centrally, thickening the lens there and increasing its power to correct the hyperopia. Similarly, to correct a myopic error postoperatively, the light pattern is more intense in the periphery of the lens. Astigmatism is corrected by shining the light in a band that crosses the lens center on the astigmatic axis.
Calhoun's Chairman, Daniel Schwartz, MD, says that multiple power adjustments to the LAL are possible until the vision is at an acceptable level. For instance, if the surgeon inadvertently adds too much thickness to the center of the lens, inducing myopia, he could irradiate the periphery to counteract it. When the patient's vision is at its best, the lens power is permanently locked in by irradiating the entire lens at once, usually a day or two after the adjustment is made. Once this is done, the power can no longer change. It's important that the patient wear UV-protective eyewear between the adjustment and lock-in steps, however, because UV light can induce a power change during this time.
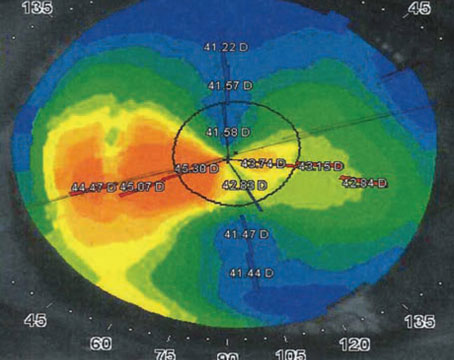
To create a multifocal effect, the company varies the spatial intensity of the light that irradiates the lens to create a central zone for distance vision and a zone for reading outside the center. This multifocal effect occurs only with the LAL's myopic adjustments so far, in which the light energy is concentrated in the periphery.
"By treating the periphery of the lens, you're basically increasing the power there and decreasing the power in the center," says
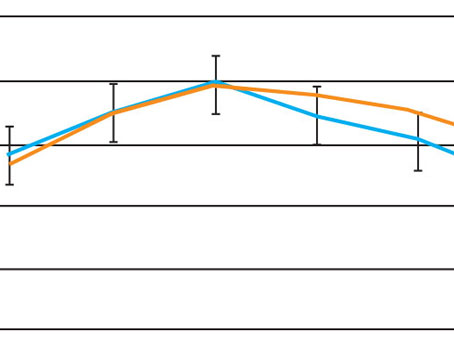
The preliminary results in 15 patients have been somewhat impressive, says Dr. Chayet, with many reading J1 and seeing 20/20 at distance. But the real benefit of the adjustment seems to be in the lack of glare and halo complaints from patients, even though such problems plagued multifocal lenses in the past.
"If you had a typical multifocal lens implant with different zones, such as one zone set for distance and the next annular zone set for near, one of the issues with that concept is that there would be zone junctions between the distance and near rings that tend to give a bit of glare," explains Chris Sandstedt, PhD, director of optics for Calhoun Vision. "With our lens, we can smoothly profile it so it's almost like a progressive lens, so you don't encounter those interfaces between zones that can cause glare and reflections that can impair a patient's contrast sensitivity."
Dr. Chayet has seen the effects of the smooth transitions in the initial few patients. "The effect of this smoothness has meant that patients basically don't complain of halos or glare," he says. "They see very naturally and don't perceive any issues between seeing things at near, intermediate or in the distance."
As to why the LAL can have smooth transitions while a manufactured multifocal lens's are rougher, Dr. Sandstedt says it has to do with the fact that a beam has a non-homogenous intensity. "We spatially profile the beam," he says. "The beam doesn't have a constant intensity across it. Unlike LASIK, which uses a spot, we irradiate the majority of the lens with a different spatial intensity in different areas; so it's different on the edges than in the middle, for example. However, we irradiate the lens with the same pattern all at once."
There exists the question of whether patients who receive a hyperopic adjustment to the LAL could receive a multifocal adjustment.
"It occurs with the myopic adjustments because of the way the spatial intensity profile is put down on the lens," Dr. Sandstedt says. "In the future, we could potentially tailor the profile such that it corrects both hyperopia and provides some sort of multifocal effect to the lens."
Since only a small number of patients with the multifocal effect have been studied so far, both Drs. Chayet and Sandstedt are quick to acknowledge that these results are just preliminary, and they say more testing is necessary to see if everyone gets the effect and how much they get. "The amount of reading vision they achieve seems to correlate with a particular spatial profile," says Dr. Sandstedt.
Dr. Chayet is planning a larger series of patients with multifocal adjustments. "The power they have for reading is variable, and the higher the adjustment the more multifocality they'll get," he says. "For example, we attempted a 2-D adjustment in one patient and he has 8 D of multifocality. He can still read J1 even if you put a -2 D lens in front of him."
The long-awaited U.S. Food and Drug Administration trial of the LAL is scheduled to begin in the fourth quarter of 2007.