Trifocal Designs and Results
European surgeons familiar with trifocal intraocular lenses say that, like many technologies, trifocals grew out of the perceived shortcomings of previous generations of devices.
Thomas Kohnen, MD, professor and chairman of the Department of Ophthalmology, Goethe University, Frankfurt, Germany, describes the forces that brought about the new lenses. “Trifocal IOLs were basically constructed because we noticed over the years that with bifocal IOLs, the the intermediate vision was not strong enough,” he says. “Patients complained about not being able to read the computer screen, and they could only read books at a very close distance or see objects in the distance—it was a major complaint. With this being the case, the idea of the trifocal lens came up, first with the FineVision lens (PhysIOL) and then with the Zeiss AT-LISA. With them, we finally had good trifocals.” Since then, the Alcon PanOptix trifocal has also entered the market.
 |
Milan, Italy’s Francesco Carones, who’s been involved with presbyopic lenses for years, and implanted the first Alcon ReSTOR toric lens in the world in 2010, says the trifocal design concepts are similar to their bifocal brethren but with a few key differences. “For multifocal IOLs, the focal distance is governed by the diffractive steps,” he explains. “So the height of the steps and the distance between them generate the second focal point. With trifocal IOLs, instead of having one single height and distance, they have two repeating steps, one for intermediate and one for near, and they can spread this pattern over the lens surface as the PhysIOL or the Zeiss lenses do.
“Within the diffractive pattern on the lens, there’s one flat area between the steps that redirects the light for distance,” Dr. Carones explains. “So, for example, for the Zeiss and the PhysIOL trifocals, the amount of light energy is 33 percent for distance vision, 33 percent for intermediate and 33 percent for near. With the Alcon PanOptix, you have 50 percent for distance, 25 percent for intermediate and 25 percent for near. The additional 25 percent it gets for distance comes from that little flat area between the double-step pattern of the PanOptix.”
The lenses differ slightly in where their focal points are set, as well. “For the PanOptix, Alcon changed the intermediate foci compared to the existing trifocal lenses,” says Dr. Kohnen. “Instead of having an intermediate vision target of 80 cm like the PhysIOL and Zeiss lenses, the company changed it to 60 cm, which it thought was more appropriate after doing research into it for intermediate distances.”
In addition to differing in the way they distribute light, these lenses also differ in their physical design, notes Florian Kretz, MD, director of Eye-Clinic Ahaus-Raesfeld-Rheine in Ahaus, Germany. “The AT-LISA is trifocal in its center and bifocal in its periphery,” he explains. “Specifically, the central 4.38 mm has a trifocal optic, and everything around it is bifocal. The near add power is 3.33 D, and the intermediate add is 1.66 D. In the periphery it’s 3.33 D near. That means that, for this type of lens, the central trifocal part is pupil-independent for light distribution, and for larger pupils the distribution changes more at near than distance in order to enhance reading acuity under dim lighting conditions.”
“The FineVision lens uses a different system,” Dr. Kretz continues. “It’s apodized over the entire surface. So the intermediate add power is 1.75 D, and the near add is 3.5 D. And due to the apodization there’s less light transferred to the intermediate and near points at the periphery, so the lens enhances far vision more the wider the pupil becomes. With this design, there’s also less straylight production.”
Finally, in
 |
There have been a couple of studies published on the PhysIOL and Zeiss lenses, but the PanOptix is newer, and so data on it is still being gathered.
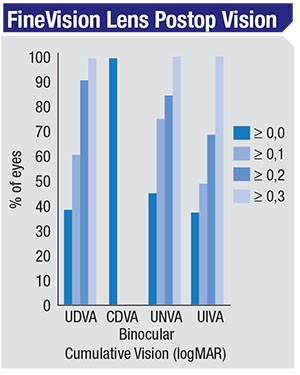
In a prospective study of the FineVision lens, Spanish researchers achieved an average binocular best-corrected distance acuity of a little worse than 20/16; a binocular distance-corrected intermediate acuity between 20/25 and 20/32; and distance-corrected near vision that was a little better than 20/25.1
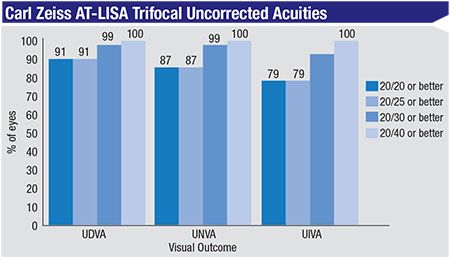
In a prospective study of the Zeiss AT-LISA lens performed by Dr. Kretz and his colleagues, all patients had a binocular uncorrected distance visual acuity of 20/20 or better and a binocular uncorrected intermediate visual acuity of 20/25 or better, three months after surgery. Furthermore, 85 percent of patients achieved a binocular uncorrected near visual acuity of 20/25 or better.2
In a non-peer-reviewed study Dr. Kretz took part in, he says that, at least preliminarily, the PanOptix lens is promising. At 12 weeks in eight binocular implantations with the PanOptix, the average uncorrected distance acuity was between 20/20 and 20/32, the average intermediate vision was between 20/20 and 20/40 and the average near vision was between 20/25 and 20/40.
When the subject of presbyopia-correcting IOLs comes up, it’s always accompanied by the shadow of photic complaints. However, reports seem to indicate these may not be worse in trifocal lenses than in bifocal multifocal IOLs. In a paper on the AT-LISA that Dr. Kretz co-authored, the mean scores (0 = no symptoms; 40 = strong symptoms) for night glare, ghost images and halos were 15.15 ±12.02, 4.49 ±7.92 and 13.34 ±10.82, respectively.3
“Among the three competitors: the Zeiss, the PhysIOL and the PanOptix,” comments Dr. Carones, “I haven’t seen significant differences in glare and halo. So I wouldn’t say this is a criterion for deciding which one to implant.” REVIEW
Drs. Kohnen and Carones are consultants to Alcon. Dr. Kretz consults for Carl Zeiss Meditec.
1. Carballo-Alvarez J, Vazquez-Molini J, Sanz-Fernandez J, et al. Visual outcomes after bilateral trifocal diffractive intraocular lens implantation. BMC Ophthalmology BMC Ophthalmol 15;26. Mar 14, 2015.
2. Kretz F, Breyer D, Diakonis V, et al. Clinical outcomes after binocular implantation of a new trifocal diffractive intraocular lens. Journal of Ophthalmology 2015;Article ID 962891:6 pages.
3. Kretz F, Choi C, Müller M, Gerl M, et al. Visual outcomes, patient satisfaction and spectacle independence with a trifocal diffractive intraocular lens. Korean J Ophthalmol 2016;30:3:180-91.


