|
Asheesh Tewari, MD |
Modern vitrectomy surgery has classically been performed with 20-ga. instruments. However, advancement in techniques and instrumentation led to the introduction of 25-ga. vitrectomy. Although this has decreased operative times and hastened postoperative recovery, some vitreoretinal surgeons have been disappointed with the inability to perform complicated surgical maneuvers due to the increased flexibility of the instruments. In response to these concerns, 23-ga. transconjunctival sutureless vitrectomy has recently been developed. In this article, we will review the principles and techniques of this new innovation in vitreoretinal surgery.
Limitations of 25-ga.
In the 25-ga. system, direct sclerotomies are placed through the intact conjunctiva with a plastic trocar used for the infusion, light pipe, and surgical instrument. At the conclusion of the case, the trocars are removed and since the incisions left in the sclera are so small, they are expected to self-seal. Advantages of this system include less postoperative astigmatism, since suturing of sclerotomies is typically not performed, and reduced conjunctival trauma and inflammatory response of the eye. Also, there is less operating time since opening and closing of sclerotomies and conjunctiva are not required.
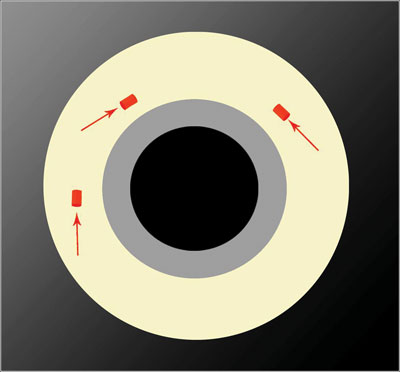 |
| Figure 1. Location of the tangential incisions made in a 23-ga. vitrectomy. All images: DORC |
Although rigidity of the 25-ga. instrumentation has improved, moving the eye using the wide-angle instrumentation can be challenging. This can become a limiting factor in removing peripheral vitreous and repairing complex retinal detachments. Removal of anterior pathology such as proliferation in diabetic retinopathy and retinal detachments with proliferative vitreoretinopathy (PVR) can be challenging since the instruments have an increased tendency to bend.
The illumination for 25-ga. has evolved with the use of chandeliers that allow for bimanual surgery and allow a wide view that may be not optimal with the standard 25-ga. light pipe. The standard light source for 25-ga. is not as bright as that of 23-ga., since there are fewer lumens available for transmission through a smaller-gauge, fiber-optic light pipe. In addition, 25-ga. sclerotomies are done directly perpendicular to the sclera and can potentially leak at the end of surgery, requiring placement of sutures in some cases. Although partial air-fluid exchange, as advocated by Steve Charles, MD, has reduced the risk of wound leakage, concerns of postoperative hypotony still remain.
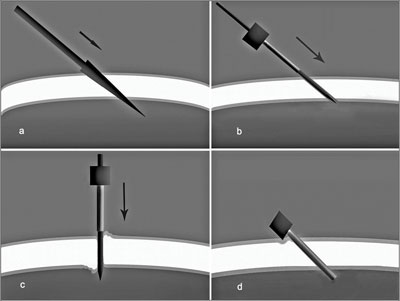 |
| Figure 2. Schematic of the tunnel-like nature of the scleral incisions. |
23-ga. Vitrectomy Technique
To alleviate issues of decreased light and rigidity, a modern 23-ga. vitrectomy system was developed.1 Twenty-three-ga. vitrectomy provides more rigid instrumentation with improved light transmission, thus allowing greater rotation of the eye and the ability to perform a more complete vitrectomy. The sclerotomies in this system are also done with a trocar transconjunctival system, but with tangential beveled self-sealing incisions with metal cannulas (See Figure 1). By making incisions at a 30-degree angle parallel to the limbus, there is greater transmural wall strength. The tunnel-like nature of these incisions facilitates the self-sealing of the wound after removal of the cannulas (See Figure 2).
The procedure is initiated by pushing the conjunctiva 2 mm laterally using a special toothed pressure plate and then holding it firmly to the sclera. A 23-ga. stiletto blade, which produces a 0.72-mm opening, is inserted at a 30-degree angle through the conjunctiva, sclera and pars plana 3.5 mm from the limbus. When placed adjacent to the limbus, the central opening of the pressure plate is 3.5 mm from the limbus. Constant pressure is applied to the pressure plate during the insertion and removal of the stiletto blade to prevent additional displacement of the conjunctiva. A blunt-tipped metal inserter with metal cannula is then inserted into the scleral tunnel and into the eye. The inserter is then removed with the aid of the notched edge of the circular pressure plate, and the metal cannula remains in place. The infusion is attached to this cannula, and then the procedure is repeated for the remaining two sclerotomies (See Figure 3). Of note, the ends of the cannulas are tapered, allowing for an easier insertion of instruments.
Illumination
Once in the eye, the illumination from the light pipe is superior to that of the 25-ga. light pipes, including the newly introduced wide-angle diffusion light pipe. This is because of the increased diameter of the 23-ga. light pipe allows greater lumens of light transmission. There are two major light pipes that can be used currently and in our experience, we have found the Total View light pipe (DORC) to be helpful in providing adequate central and peripheral visualization of the retina. Brighter light makes surgical manipulation of the vitreous and retina easier. Also, decreased illumination from smaller light pipes has been linked to missing intraoperative retinal breaks that can lead to postoperative retinal detachments.2
Increased Rigidity of Instrumentation
Once vitrectomy has begun, the rigidity of the instruments is quite noticeable. With its increased diameter compared to 25-ga., the 23-ga. vitrector has been described as having a similar feel to 20-ga. instruments (See Figure 4). With 23-ga., the eye can be easily rotated to access peripheral vitreous and retinal pathology. Additionally, with wide-angle viewing systems, peripheral shaving of the vitreous base can be performed. Also, anteriorly located pathology can be accessed without bending of the instruments. Overall, a more thorough vitrectomy can be performed. This is important because a remaining large peripheral vitreous skirt can be associated with a certain degree of vitreoretinal traction and can be associated with retinal tears and detachments in the postoperative period. This has been reported in 25-ga. vitrectomy, where the postoperative retinal detachment rate was approximately 2 percent.3
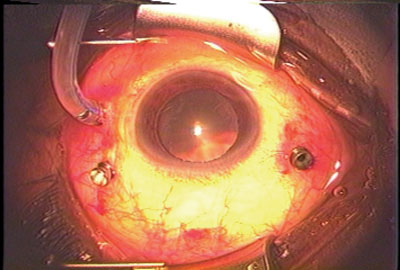 |
| Figure 3. Metal cannulas in place for a 23-ga. vitrectomy. |
A full complement of instruments is available for 23-ga. system, including end-gripping forceps, intraocular scissors, flute needle, endodiathermy probe, and endolaser probes. Just like 25-ga. instrumentation, as this new technology develops further, there will likely be more instrumentation produced by the many ophththalmic manufacturers.
Fluidics
High-speed vitreous cutters have allowed for safer and more efficient shaving of the vitreous base. With lower aspiration and higher cut rates, there is less traction placed at the vitreous base during cutting, and the risk for retinal tears is reduced. With 25-ga. systems, the flow rate is reduced, owing to the smaller diameter available for flow. As defined by Poiseuille's equation, rate of flow through a tube is proportional to the radius of the tube to the fourth power. This explains why greater flow rates can be achieved with the 23-ga. system, and it is with improved flow rates that certain parts of the vitrectomy, such as removing the posterior hyaloid, can be done effectively and efficiently.
Postoperative
Once vitrectomy is complete, the cannula is removed by engaging it with specially designed forceps and pulling them directly out, followed by gentle pressure over the incision site with a cotton-tipped applicator. Although there can be some small subconjunctival hemorrhage from episcleral and conjunctival vessels, this usually resolves within a few days after surgery. Since the incisions are angled, the scleral wound is pressed together by the intraocular pressure. Preliminary data has revealed no cases of decreased IOP on postoperative day one.1 Also, since sutures are not used, there is minimal induced postoperative astigmatism.
 |
| Figure 4. Size comparison of 20-ga., 23-ga. and 25-ga. vitrectors (from left to right). |
The 25-ga. system involved perpendicular incisions through the sclera. When those trocars are removed, an open hole in the sclera is often clearly visualized and represents a direct opening from the vitreous to the outside of the eye. This can put the patient at a theoretically increased risk for endophthalmitis. Also, openings in the sclera can be associated with wound leakage. Previously reported series of 25-ga. vitrectomies have demonstrated wound leakage requiring suture placement in 7 percent of cases.4 Hypotony in the postoperative period can increase the risk for complications, including retinal and vitreous incarceration and suprachoroidal hemorrhage.
There has always been progressive advancement in the technology and instrumentation that vitreoretinal surgeons have used since Robert Machemer first introduced vitrectomy surgery in the 1970s. Twenty-five-ga. surgery paved the way for small incision surgery, and 23-ga. transconjunctival sutureless pars plana vitrectomy represents the latest innovation in vitreoretinal surgery. Twenty-three-ga. surgery involves beveled, sutureless scleral incisions that are less likely to leak, larger-diameter instruments with increased rigidity, improved light illumination, and the overall ability to perform a more complete vitrectomy, which can lead to decreased operative time and improved surgical outcomes for our patients. Although 25-ga. surgery is a good option for many surgeons, 23-ga. vitrectomy is an additional tool in the armamentarium of the vitreoretinal surgeon.
Dr. Tewari is a vitreoretinal fellow at the Barnes Retina Institute, Washington University Department of Ophthalmology and Visual Science. Dr. Shah is from the Barnes Retina Institute and is a clinical associate professor with Washington University Department of Ophthalmology and Visual Science.
Contact Dr. Shah at Barnes Retina Institute, 1600 S. Brentwood Blvd., Suite 800, St. Louis, M0, 63144. Phone: (314) 367-1278, fax: (314) 962-2770, E-mail: gkshah1@gmail.com.
1. Eckardt C. Transconjunctival sutureless 23-gauge vitrectomy. Retina 2005;25:208-11.
2. Fujii GY, De Juan E Jr., Humayun MS, et al. A new 25-gauge instrument system for transconjunctival sutureless vitrectomy surgery. Ophthalmology 2002; 109:1807-12.
3. Ibarra MS, Hermel M, Prenner JL, Hassan TS. Longer-term outcomes of transconjunctival sutureless 25-gauge vitrectomy. Am J Ophthalmol 2005;139:831-6.
4. Lakhanpal RR, Humayun MS, De Juan E Jr., et al. Outcomes of 140 consecutive cases of 25-gauge transconjunctival surgery for posterior segment disease. Ophthalmology 2005;112:817-24.


